



Chronic Occlusion of the Superior Vena Cava
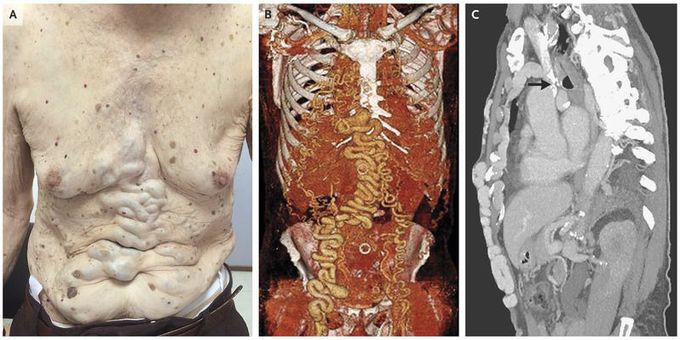
An 89-year-old man presented to the outpatient clinic for evaluation of a right inguinal hernia. He had a history of hypertension and also reported having abdominal-wall varices that had been increasing in size for 20 years. He had no history of central venous catheterization. On physical examination, marked venous dilatation was apparent on the abdomen (Panel A). Computed tomographic (CT) angiography revealed collateral circulation through anastomoses between the subcutaneous veins and the common femoral veins, particularly on the right side (Panel B). The superior vena cava was occluded in its distal portion, as seen in a CT scan (Panel C, arrow), and the azygos vein was obstructed at the level of the carina. The inferior vena cava was patent. Obstruction of the superior vena cava can be caused by extrinsic compression (e.g., from a compressing mass) or by inflammation or scarring of the vessel (e.g., from repeated placement of central venous catheters, fibrosing mediastinitis, or infection). Chronic occlusion may lead to the formation of collateral veins to maintain venous flow. In this patient, the cause of the chronic occlusion was not definitively determined. The patient was lost to follow-up before elective surgery could be performed. He presented 5 months later with an incarcerated right inguinal hernia and died from postoperative complications of emergency surgery.

