



Congenital Cytomegalovirus Infection
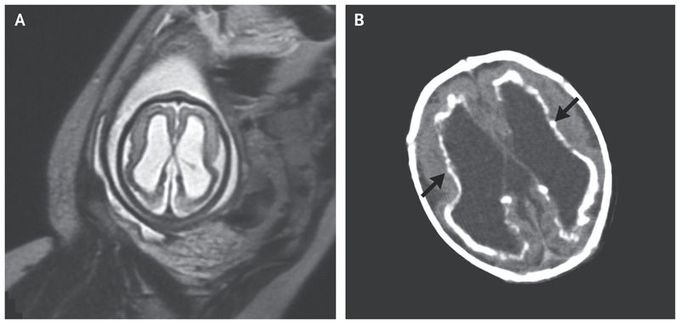
A 35-year-old woman presented to the obstetrical clinic for routine fetal ultrasonography at 24 weeks of gestation. Her medical history was notable for a febrile illness that had occurred shortly after conception. Ultrasonographic images showed ventricular dilatation in the fetal brain, and T2-weighted magnetic resonance imaging revealed ventriculomegaly (Panel A) and cerebellar hypoplasia. Maternal serum immunoassay was positive for cytomegalovirus (CMV) IgG and IgM antibodies. At 38 weeks of gestation, the woman had a normal vaginal delivery of a male baby weighing 2556 g (8th percentile) with a head circumference of 30.5 cm (1st percentile). Petechiae were observed on the newborn’s face and trunk. Laboratory evaluation revealed a platelet count of 136,000 per cubic millimeter (reference range, 150,000 to 450,000) and normal hematocrit and aminotransferase levels. Computed tomographic scans of the newborn’s brain showed ventricular dilatation, parenchymal hypoplasia with polymicrogyria, and periventricular calcifications (Panel B, arrows). Immunohistochemical testing of the placenta was positive for CMV, and polymerase-chain-reaction testing of the newborn’s urine revealed CMV DNA — findings that confirmed congenital CMV infection. Congenital CMV infection can be asymptomatic, or symptoms can include growth restriction, hematologic disorders, and sensorineural developmental disorders that range in severity from mild to severe. The newborn was treated with ganciclovir. At a follow-up visit at 11 months of age, the child had sensorineural hearing loss in the right ear, epilepsy, spastic quadriparesis, and developmental delay; treatment included antiepileptic medication and developmental services.
