



Acute Human Immunodeficiency Virus Infection
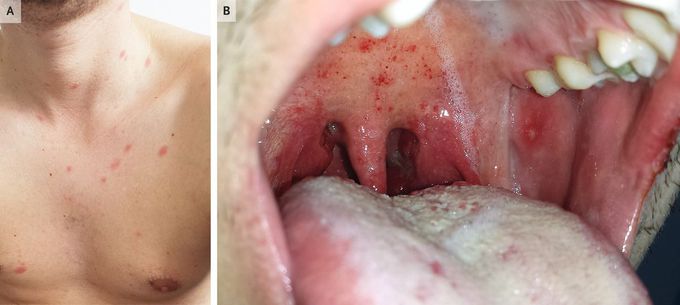
A previously healthy 26-year-old man presented to the emergency department with a 5-day history of an asymptomatic rash, sore throat, fevers, chills, and malaise. On physical examination, scattered, erythematous papules and macules could be seen across the upper chest and anterior neck (Panel A). In the mouth, palatal petechiae, buccal mucosal ulcerations, and pharyngeal erythema were observed (Panel B). There was no palpable lymphadenopathy. Laboratory testing showed leukopenia, lymphopenia, mild thrombocytopenia, and an elevated C-reactive protein level. Tests for several respiratory viral pathogens, Epstein–Barr virus, measles, rubella, and syphilis were negative. A rapid antibody test for human immunodeficiency virus (HIV) was negative. However, a subsequent fourth-generation combination HIV antigen and antibody test was positive, and the HIV viral load was greater than 10 million copies per milliliter (reference value, undetectable). A diagnosis of acute HIV infection was made. The patient reported having had condomless sex with a new partner 2 weeks before presentation. In acute HIV infection, HIV antibodies do not form until several weeks after infection, whereas HIV viremia and the p24 antigen are detectable much earlier. Antiretroviral therapy was started, and the patient’s symptoms rapidly abated.

Living with HIV was one of the hardest experiences of my life. The fatigue, the emotional toll, and the uncertainty about the future weighed on me every single day. I had tried many treatments and medications, but nothing seemed to restore my health or energy the way I hoped.Out of both hope and desperation, I came across NaturePath Herbal Clinic. At first, I was skeptical but something about their natural approach and the powerful stories I read gave me the courage to try one more time.I began their herbal treatment program, and within a few weeks, I noticed small but meaningful changes more energy, better sleep, and a stronger immune system. Over the months, those improvements only grew. Today, I can truly say my life has changed. I feel healthier, more balanced, and finally in control of my well-being again.This isn’t just a testimony it’s a heartfelt recommendation to anyone living with HIV or any chronic condition. Don’t give up hope. I’m so grateful I gave NaturePath Herbal Clinic a chance. Visit their website to learn more: www.naturepathherbalclinic.com Email: info@naturepathherbalclinic.com

RECOVERY LOST BITCOIN FROM TRADING PLATFORM CONTACT: GEO COORDINATES RECOVERY HACKER I would love to extend my gratitude and utmost appreciation to Geo Coordinates Hacker for helping me recover my money back. They helped me recover my stolen money, 634,000 dollars worth of bitcoin effortlessly. Their service is not only quick but professional and reliable. As someone who was skeptical about the process, I was pleasantly surprised to see my bitcoins returned in such a swift and hassle-free manner. Geo Coordinates Hacker truly goes above and beyond to ensure their clients' satisfaction. I would highly recommend Geo Coordinates Hacker for all your cryptocurrency recovery, digital funds recovery, hacking, and cybersecurity-related issues. Without a doubt, they are the best and I am very grateful to them for helping me recover my money. In case you have the same issues related to mine do not hesitate to reach out to them through their email Contact; Email: geovcoordinateshacker@gmail.com Website; https://geovcoordinateshac.wixsite.com/geo-coordinates-hack
