



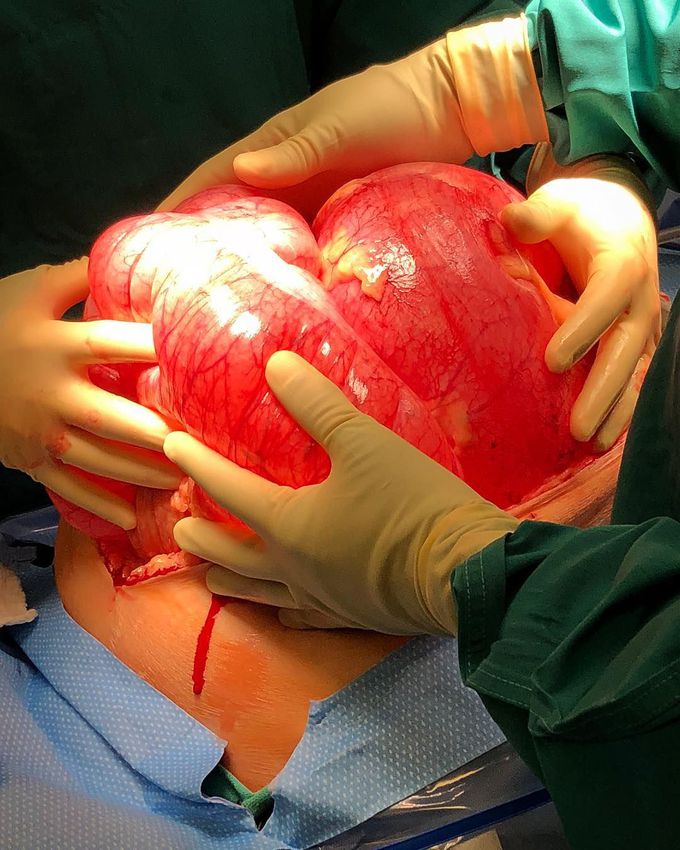
A megacolon from sigmoid volvulus!!
The image above shows a greatly dilated sigmoid colon that almost fills the entire abdomen! The patient presented with large bowel obstruction symptoms - constipation, abdominal bloating, nausea and vomiting, with marked abdominal distention on examination. Intraoperatively, sigmoid volvulus was found to be the cause of his intestinal obstruction. This condition occurs when the sigmoid colon twists around itself and its narrow and elongated mesentery and, not surprising, the intestinal obstruction risk rises when twisting of the intestines is more than 180 degrees with the sigmoid involved in up to 90% of cases. Plain abdominal radiography showing the dilated loops often with a few air-fluid levels is used to diagnose the volvulus in most cases with CT scan or MRI as the confirmatory tests when necessary. Surgically, after the colon has been untwisted, the definitive and standard therapy is sigmoid resection and primary anastomosis. A nonresective alternatives is also widely used with mixed success. Rapid surgical involvement is mandatory to prevent complications such as hemorrhagic infarction, perforation, septic shock, and death. Photo by @drbuckparker
Midgut volvulus (midgut= lower duodenum to the proximal 2/3 of transverse colon) is more common in infant and children while sigmoid ie hindgut volvulus is more common in elderly

