



Tubular Opacities in the Gastrointestinal Tract
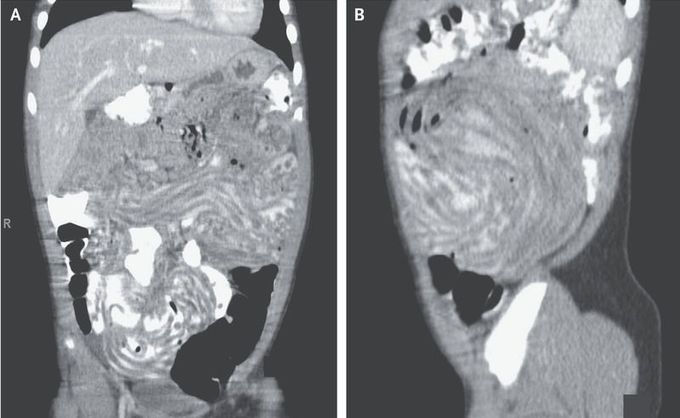
A 3-year-old boy presented to the emergency department with a 6-month history of intermittent postprandial abdominal pain and vomiting. He had returned from Senegal 8 months before presentation. On two previous occasions since his return, he had presented with similar symptoms, which were attributed to viral gastroenteritis. On examination, he appeared well, with normal vital signs. An abdominal radiograph showed a nonobstructive bowel gas pattern with thickened colonic haustra. Computed tomography of the abdomen with contrast enhancement showed a large burden of tubular structures filling the small bowel (Panels A and B) — a finding consistent with infection with Ascaris lumbricoides. Examination of the stool for ova and parasites revealed infection with A. lumbricoides, as well as coinfection with Trichuris trichiura. A. lumbricoides and T. trichiura are helminths that are transmitted by ingestion of contaminated soil, food, or water. Helminth infection should be considered in patients with gastrointestinal symptoms who have resided in or traveled to regions in which such infections are endemic. The patient received a course of albendazole and subsequently passed worms in his stool over the course of 7 days. His symptoms resolved after completion of the treatment, and he had no recurrence of abdominal pain.
