



Liver Involvement in Autosomal Dominant Polycystic Kidney Disease
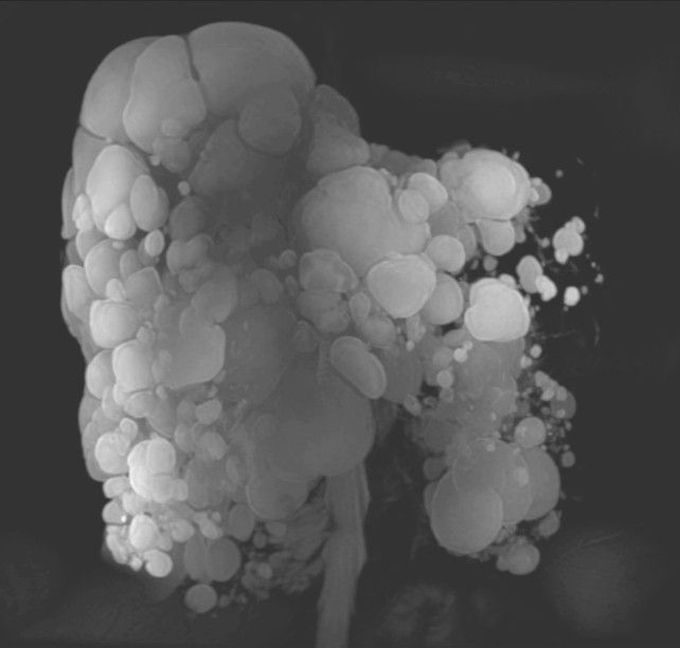
A 51-year-old woman with autosomal dominant polycystic kidney disease presented to the primary care clinic with mild worsening of chronic abdominal pain. No jaundice was found on physical examination; the liver was enlarged, and the patient had mild tenderness in the right upper quadrant and in the flanks on both sides. Murphy’s sign was absent. Laboratory studies showed mildly elevated levels of aspartate aminotransferase and alanine aminotransferase. Innumerable cysts were found on abdominal ultrasonography; the gallbladder could not be visualized. Magnetic resonance cholangiopancreatography was performed and revealed a markedly enlarged liver with numerous cystic structures (a three-dimensional maximum-intensity-projection reconstruction is shown in the figure). No signs of intracystic hemorrhage, rupture, or infection were found; the presentation was not consistent with acute cholecystitis. In autosomal dominant polycystic kidney disease, cysts can develop in a range of sites, including the liver, pancreas, and seminal vesicles. The patient was treated with intravenous hydration and analgesia, and the pain decreased. At a 1-year follow-up visit, no additional complications or new symptoms had developed. The patient continued to have occasional abdominal pain.

It's a genetic predisposition. Polycystic kidneys, ovaries, liver, are all genetic diseases. Meaning, it is passed down generation to generation. All of these organs are in the abdomen.
The cause of most liver cysts is unknown.Liver cysts can be present at birth or candevelop at a later time. They usually grow slowly and are not detected until adulthood. Some cysts are caused by a parasite, echinococcus that is found in sheep in different parts of the world.
When we have to treat for this condition??and If we didn't treat now it gets complicated and is the patient end up in endstage liver disease ??
