



Pituitary Hyperplasia from Primary Hypothyroidism
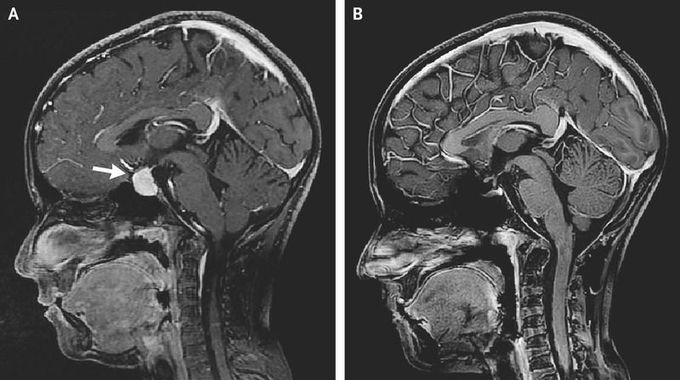
A 10-year-old girl presented to the pediatric clinic with headache and poor growth. On examination, her height was below the third percentile and her weight was at the tenth percentile. She had dry skin; testing showed no visual-field deficits. Laboratory studies showed a thyrotropin level of more than 150 μU per milliliter (normal range, 0.5 to 4.9), a free thyroxine level of 0.4 ng per deciliter (5.1 pmol per liter) (normal range, 0.8 to 1.4 ng per deciliter [10.3 to 18.0 pmol per liter]), and a prolactin level of 63 ng per milliliter (normal range, 3 to 28). The results of additional testing, which included the evaluation of levels of morning cortisol, gonadotropins, and insulin-like growth factor 1, were normal. Magnetic resonance imaging (MRI) of the head revealed a diffusely enhancing lesion in the sellar region extending to the optic chiasm (Panel A, arrow). A diagnosis of primary hypothyroidism with secondary pituitary hyperplasia was made, and the patient began receiving levothyroxine. Long-standing untreated primary hypothyroidism can cause pituitary hyperplasia owing to hormonal-feedback mechanisms through the hypothalamic–pituitary–thyroid axis. At 10 months of follow-up, the patient’s headaches had resolved, the thyrotropin level had normalized, and the patient had grown 6 cm in height. Repeated MRI of the head showed resolution of the pituitary enlargement (Panel B).
