



Lemierre’s Syndrome
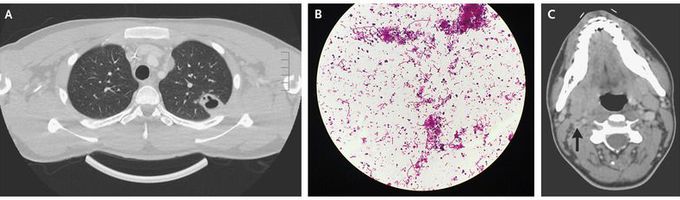
An 18-year-old man presented to the emergency department with a 1-week history of sore throat, fever, and malaise and a 3-day history of pleuritic chest pain and productive cough. He reported no history of intravenous drug use, recent travel, or known sick contacts. On examination, he was febrile and ill-appearing and had an oxygen saturation of 88% while breathing ambient air. A chest radiograph showed consolidation in the middle and upper portions of the left lung, and computed tomography of the chest revealed multiple cavitary lesions (Panel A) and a loculated left pleural effusion. An anaerobic blood culture obtained at the time of admission grew Fusobacterium necrophorum (Panel B). Contrast-enhanced computed tomography of the neck revealed an intraluminal filling defect in the right internal jugular vein, a finding suggestive of thrombus (Panel C, arrow). Lemierre’s syndrome was diagnosed. Lemierre’s syndrome is characterized by thrombophlebitis of the internal jugular vein and evidence of disseminated infection (often septic pulmonary emboli), typically after a recent oropharyngeal infection. The patient underwent drainage of the pleural effusion and received intravenous ceftriaxone and oral metronidazole. At follow-up after the completion of antimicrobial therapy, he had recovered well.
Thank you for sharing Lemierre’s Syndrome; it’s a horrible infection represented by an anaerobe. Thank you for stating the young man pulled through, and thanks to outstanding MD’s for their exemplary efforts.
