



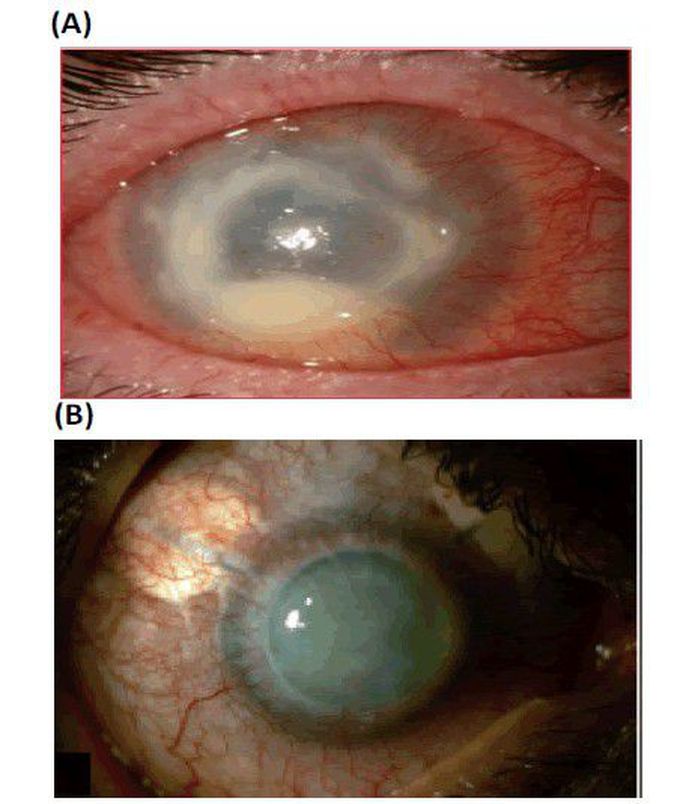
Infected eye
Treatment and Case Studies Acanthamoeba is difficult to treat, but effective management can save ones eye. Topical anti-infective agents used in early-stage, surgical intervention is necessary in later stages. Propamidine 0.1% and neomycin 1% shows good activity against AK Since then, two or more topical anti-amoebic agents are used throughout the day. Polyhexamethylene Biguanide (PHMB, 0.02%) and chlorhexidine (0.02%), are effective in both monotherapy and combination therapy with a diamidine [13]. Case studies show that the Acanthamoebakeratitis is successfully treated in the person having the contact lens using six month therapy with topical Miconazole, Metronidazole, Prednisolone and neomycin as well as oral ketokonazole. In another case of person without contact lens having burning sensation the additional use of Propamidine in the above therapy shows the improvement in the corneal ulcer. In another case where topical Tobramycin and Cefazolin added in the therapy [14]. The combination of Dibromopropamidine and Propamidine isethionate ointment and drops and neomycin drops are used successfully in the 44 years old patient having corneal infection from Acanthamoeba species [15]. Bilateral Acanthamoeba keratitis was successfully treated with Chlorhexidine, Polyhexamethylene biguanide, Propamidine ise-thionate in combination with Atropine and Dibromopropamidine an improvement was noted at which point Atropine and Dibromopropamidine were stopped while Fluorometholone acetate, Acyclovir and Ciprofloxacin were prescribed and patient was discharged [16]. Few studies state that addition of the neomycinpolymyxin B also gives the good result [17]. Prevention Mostly the Contact lens wearers need to take precaution while cleaning the lenses should never use the tap water and saline to clean. As the treatment is toxic and lengthy so they should visit if they find out some sign of inflammation. And those without lenses they should not wash their eyes with lake or sea water.
