



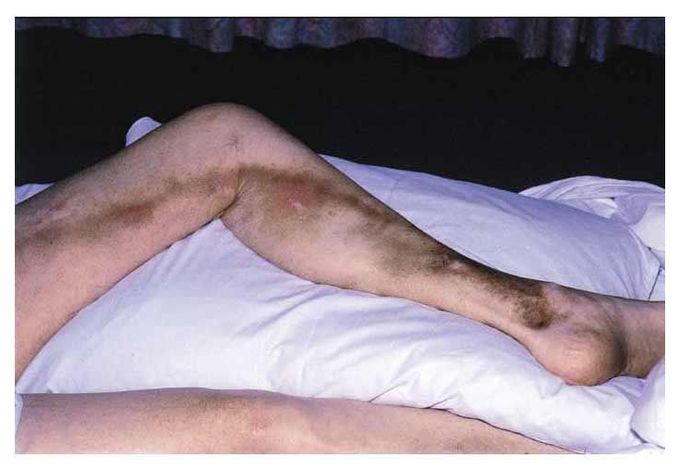
Superficial Thrombophlebitis
A 56-year-old woman began to have pain and redness of the left leg the day after a six-hour car ride. Two days later she was found to have erythema and tenderness on the medial aspect of the left knee and moderate pitting edema of the left ankle. The remainder of the examination was unremarkable. She had no history of deep venous thrombosis. Both her parents, however, had a history of deep venous thrombosis. Despite treatment with warm compresses, aspirin, and elevation of the leg, the pain and erythema increased. A palpable, ropelike cord was present from the left medial malleolus to the groin. Duplex Doppler ultrasonography revealed thrombosis of the greater saphenous vein, with no extension into the deep venous system. Despite anticoagulation with heparin, a vague, substernal chest pain developed that was unrelieved by nitroglycerin. Cardiac enzymes, electrocardiographic findings, and arterial blood gas levels remained normal. The results of ventilation–perfusion scanning were indeterminate for pulmonary embolism, and a pulmonary arteriogram was negative. Repeated duplex Doppler ultrasonography 5, 10, and 25 days after presentation showed no extension of the thrombus into the deep venous system. Studies revealed that the patient had lupus anticoagulant, and a diagnosis of primary antiphospholipid-antibody syndrome was made. Other studies for thrombophilic tendencies, including tests for factor V Leiden and protein C and S deficiencies, were negative. Two weeks after the initiation of treatment with warfarin, the international normalized ratio was 3.4 and the patient's symptoms had resolved. Follow-up at three months showed no recurrence. Michael A. Lucia, M.D. University of Nevada School of Medicine, Reno, NV 89520-0111 E. Wesley Ely, M.D., M.P.H. Vanderbilt University Medical Center, Nashville, TN 37232-8300 Source: nejm.org
There is an extensive list of causes to superficial thrombophlebitis ranging from buergers disease, varicose, obesity, age, drugs,. APLA, Factor V leiden, Protein C and S, Homocysteinemia, malignacies, metabolic disorders etc. Hence involves an exhaustive workup. About 5.5% of patients have Protein C deficit. The basic workup always includes a complete count with APLA, Prtn C and S, Factor V leiden and Antithrombin III. Management involves anticoagulant therapy with pain relievers and warm compresses. Compression stockings are also recommended. Long term monitoring required.


Living with Lupus is often a battle not just against the illness itself, but also against the emotional weight of uncertainty, fatigue, and the toll of long-term medications. For one courageous woman, that battle began in 2013. Diagnosed after Lupus had already affected her joints and internal organs, she was quickly placed on medication that initially helped. But as time went on, her health declined again this time with more frequent flare-ups and increasingly difficult side effects. Like many others with chronic illness, she faced the crushing weight of hopelessness. Each day became harder than the last, and conventional treatments no longer offered the comfort they once did. But in March 2020, at her lowest point, she made a decision that changed everything.Out of desperation and with a healthy dose of skepticism she turned to NaturePath Herbal Clinic, hoping their natural Lupus treatment might offer at least some relief. What happened next went far beyond her expectations.After completing a six-month herbal program, her flare-ups stopped entirely. Her energy returned. The chronic pain that had defined her daily life began to fade. For the first time in years, she felt like herself again. Not just alive but truly living.Her story is not just one of healing; it’s one of resilience, open-mindedness, and the courage to try something new when all else fails. By sharing her journey, she hopes to offer something priceless to others living with Lupus: hope.This treatment has been a true breakthrough for her. If you’re searching for a safe, natural, and effective alternative, I genuinely recommend giving this a chance.”www.naturepathherbalclinic.com or email them at info@naturepathherbalclinic.com
