



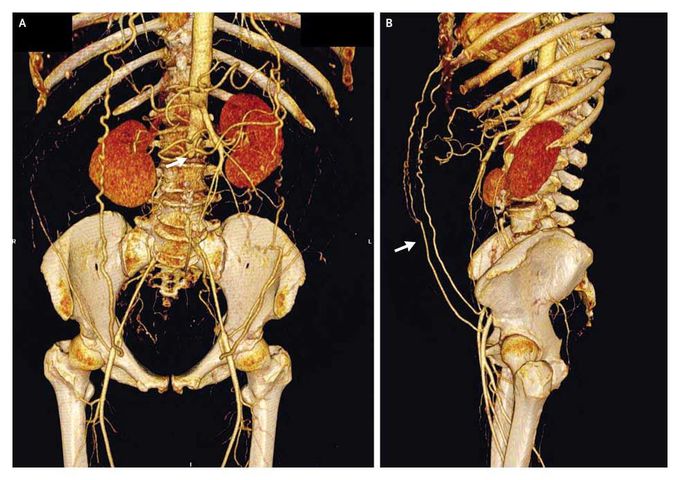
Infrarenal Aortic Occlusion
A 55-year-old woman awoke with an acute onset of bilateral leg numbness and weakness. Initial evaluation and lumbar magnetic resonance imaging, which was performed to assess the patient for disk disease, showed no cause for her symptoms, but her ankle pulses were noted to be diminished. The patient smoked cigarettes and had untreated hyperlipidemia; she reported that during the previous year, she had had bilateral buttock and thigh pain on walking 300 m. Her renal function was normal. Computed tomographic angiography showed complete occlusion of the infrarenal abdominal aorta (Panel A, arrow). A lateral view showed collateral blood flow from both internal thoracic arteries through subcutaneous epigastric abdominal vessels to the external iliac arteries (Panel B, arrow). Treatment included antiplatelet and statin therapy, successful smoking-cessation intervention, and exercise rehabilitation for peripheral artery disease. At 4 months, the patient's pain-free and maximal walking distances had improved. Distal aortic occlusion occurs most commonly in young women with dyslipidemia who smoke. Aortic atherosclerosis (a chronic process) with subsequent aortic occlusion (an acute thrombotic process) can occur without major threat to leg survival and function when collateralization is extensive, as was the case in this patient. Medical therapy can be effective, thus avoiding the risk of surgical revascularization. At her last visit, the patient had not required revascularization and was able to perform normal activities of daily living. Alan T. Hirsch, M.D. Michael D. Miedema, M.D. Abbott Northwestern Hospital, Minneapolis, MN 55407 source: nejm.org
