



Renal Artery Thrombosis in Essential Thrombocythemia
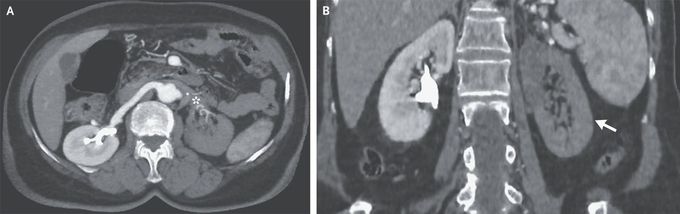
A 73-year-old woman presented to the emergency department with a 2-day history of left flank pain. She had no cardiovascular risk factors or history of tobacco use. Her body temperature was 38.5°C. Findings from a physical examination were normal. Laboratory testing was notable for a platelet count of 652,000 per cubic millimeter (reference range, 150,000 to 400,000) with an otherwise normal complete blood count. No previous platelet count was available. The lactate dehydrogenase level was 422 U per liter (reference range, 100 to 250). Computed tomography of the abdomen with intravenous contrast material showed a filling defect in the left renal artery (Panel A, asterisk) and a perfusion defect in the left renal cortex (Panel B, arrow) — findings that were consistent with an occlusive thrombosis of the left renal artery and associated renal infarction. Further testing revealed no evidence of cardioembolic disease, renal artery injury, or inherited thrombophilia. Owing to a persistently elevated platelet count, genetic testing was performed for the JAK2 V617F variant, and the result was positive. A diagnosis of essential thrombocythemia was made. Essential thrombocythemia may be complicated by arterial or venous thrombosis. The goal of treatment in patients with this condition is the prevention of vascular events. Treatment with hydroxyurea and aspirin was initiated. At follow-up 2 months later, the patient felt well and the platelet count was normal.
