



Chronic Nitrofurantoin-Induced Lung Injury
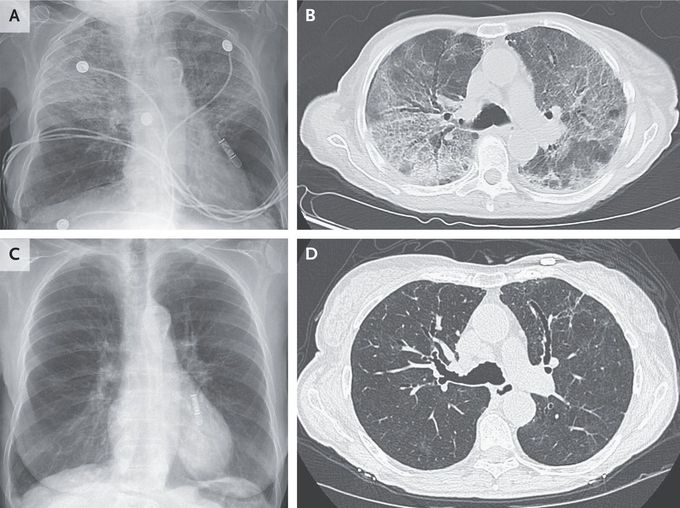
A 95-year-old woman presented to the emergency department with a 4-week history of dyspnea and dry cough. She had not previously reported these symptoms to her doctor. She reported no fevers. For the past 6 months, she had been taking nitrofurantoin daily to prevent recurrent urinary tract infections. Her oxygen saturation was 83% while she was breathing ambient air. On physical examination, inspiratory crackles were noted in the upper lung fields. There was no jugular venous distention or edema. Laboratory studies showed neutrophilic leukocytosis but no eosinophilia or elevations in aminotransferase levels. A chest radiograph was notable for patchy alveolar opacities that were most prominent in the upper lobes (Panel A). A sputum culture and viral respiratory panel were negative. A subsequent computed tomographic image of the chest showed ground-glass and reticular opacities with upper-lobe predominance and moderate bronchiectasis (Panel B). Owing to the patient’s imaging findings and long-term nitrofurantoin exposure, a diagnosis of chronic nitrofurantoin-induced lung injury was made. In patients with nitrofurantoin-induced lung injury, the radiologic findings are varied and may be diffusely distributed or localized. Treatment with nitrofurantoin was stopped, and a prednisone taper was prescribed. One week later, the patient’s symptoms had abated. Two months later, repeat imaging showed that the opacities had nearly resolved and the bronchiectasis had stabilized (Panels C and D, respectively).
