



Untreated Chronic Gout
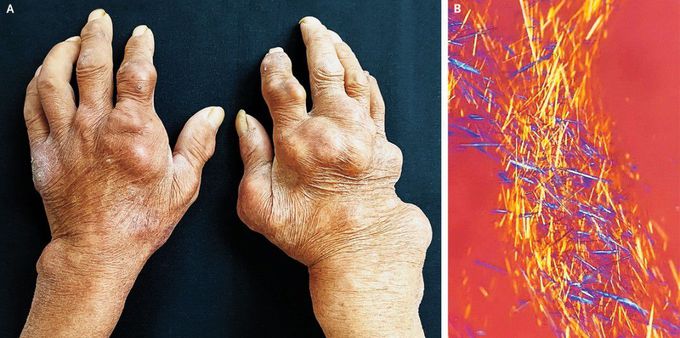
A 65-year-old man with gout and chronic kidney disease presented to the dermatology clinic with a 5-year history of joint pain and swelling in his hands, feet, and knees. During these 5 years, he had intermittently received medical therapy for gout and had had associated periods of transient improvement; however, he did not consistently receive long-term medications, and his arthritis progressed. On physical examination, he had multiple tophi and deformities in the joints of his hands (Panel A), feet, and knees. He was referred to the rheumatology clinic for further evaluation and treatment. Laboratory studies showed a serum urate level of 9.6 mg per deciliter (570 μmol per liter; reference range, 3.5 to 7.0 mg per deciliter [210 to 420 μmol per liter]) and a serum creatinine level of 1.8 mg per deciliter (160 μmol per liter; reference range, 0.7 to 1.2 mg per deciliter [60 to 110 μmol per liter]). Arthrocentesis of the first metatarsophalangeal joint of his right foot yielded a viscous, white exudate; numerous monosodium urate crystals were visible under polarized light microscopy (Panel B). Urate-lowering therapy was initiated. At 10 months of follow-up, the patient’s joint pain and swelling had abated markedly.
