



Pacemaker-Associated Superior Vena Cava Syndrome
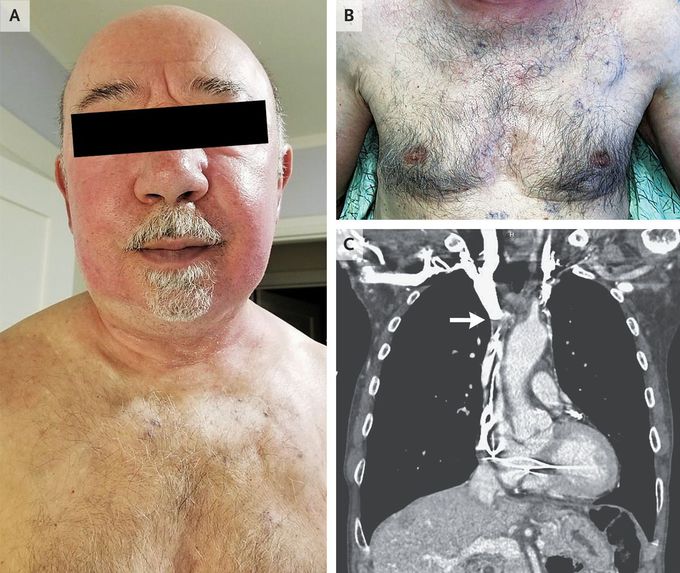
A 75-year-old man presented to the dermatology clinic with erythema of the face. He had recently started a new medication, mirtazapine, and was concerned about a possible drug reaction. However, he also noted a 1-month history of progressive swelling of the face and arms, along with dizziness with position changes. His medical history was notable for sick sinus syndrome, for which he had undergone placement of a pacemaker 8 years earlier. Two years before the current presentation, the pacemaker leads had been replaced after a lead had fractured. The physical examination was notable for erythema and edema of the face and neck, with mild cyanosis of the lips (Panel A), diffuse varicosities across the anterior chest (Panel B), edema of both arms, and distended jugular veins. Radiography of the chest showed a dual-chamber pacemaker with appropriately positioned transvenous leads. Subsequent computed tomographic venography of the chest revealed occlusion of the upper superior vena cava caused by thrombus encasement of the transvenous leads (Panel C, arrow) and extensive venous collateral vessels within the lower neck and superior mediastinum. The patient was admitted to the hospital, and intravenous heparin was initiated. A month later, he underwent pacemaker extraction with placement of a leadless system. At follow-up 3 days after the procedure, his symptoms had resolved.
