



Kartagener’s Syndrome
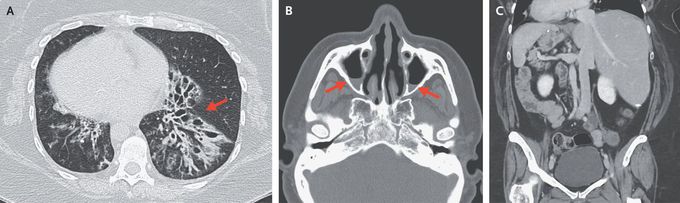
A 46-year-old woman with Kartagener’s syndrome presented to the primary care clinic with a 2-week history of fevers, worsening productive cough, and shortness of breath. In the clinic, she was afebrile and had an oxygen saturation of 95% while breathing ambient air. The examination was notable for rales and expiratory wheezing in both lungs. Computed tomography (CT) of the chest showed bronchiectasis in both lower lobes, with tree-in-bud nodularity. Bronchiectasis was most prominent in the lower left lobe (Panel A, arrow). Known dextrocardia was also noted. Sputum cultures grew Pseudomonas aeruginosa; treatment with levofloxacin was initiated, and the cough, shortness of breath, and fevers resolved. Two months later, facial pain developed, and CT of the head showed findings consistent with acute sinusitis with maxillary sinus air–fluid levels (Panel B, arrows), as well as chronic mucosal thickening. The patient’s symptoms again abated after antibiotic treatment. A previous abdominopelvic CT had shown situs inversus totalis (Panel C). Kartagener’s syndrome, a subtype of primary ciliary dyskinesia, is characterized by the triad of situs inversus, chronic sinusitis, and bronchiectasis. The syndrome is also associated with infertility. This patient continues to follow up with a multidisciplinary team.
