


Wound skin closures
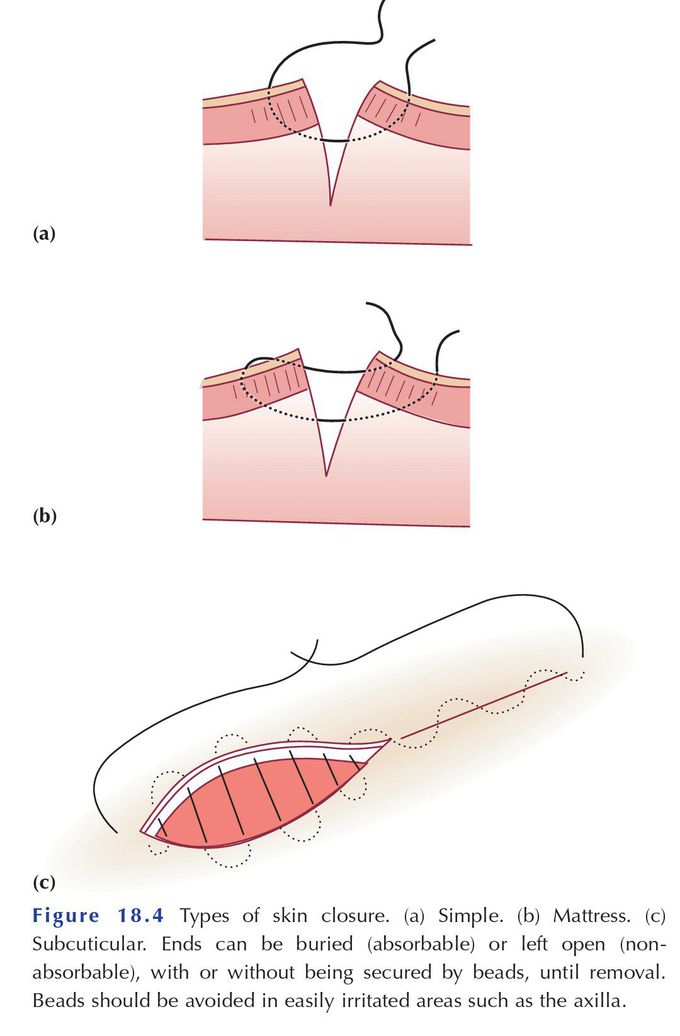
Skin closure may be interrupted or continuous; or simple, mattress or subcuticular. Interrupted sutures have the advantage that they can be removed individually, if a haematoma or infection forms locally, to help drain blood, or pus if a wound abscess develops later, without disruption of the whole suture line. They are disadvantaged by being slower to insert than continuous sutures. Mattress sutures appose skin edges tidily, ensure eversion and help to close the dead space in the subcutaneous fat layer. They are slower to insert than simple sutures but may avoid the need for a ‘fat stitch’ before closing skin. This ‘fat stitch’ may leave a poor cosmetic result; for example, after excision of a breast lump (when placed to close dead space and theoretically reduce the risk of haematoma), it may, through attachment to a breast compartment ligament, cause a permanent dimpling effect in the skin. Subcuticular sutures are cosmetically appealing but are more difficult to place in a wound that is curved. Any dead space in the subcutaneous fat layer may also need to be closed separately (but see the caution above in breast skin closure). Nevertheless, subcuticular closure is the most widely practised skin closure in virtually all specialties, although skin clips have their advocates.
