



Hemolytic Anemia after Mitral-Valve Repair
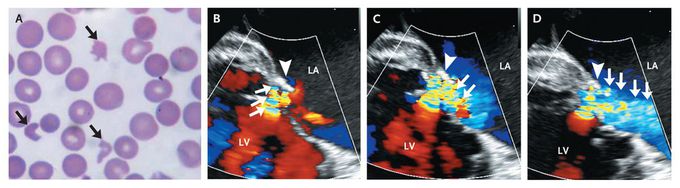
An 80-year-old woman with a history of mitral-valve repair presented with fatigue. On examination, she had normal vital signs and markedly pale conjunctivae. A grade 3/6 pansystolic murmur was audible at the apex, with radiation to the back. The hemoglobin level was 8 g per deciliter. Hematologic studies revealed indirect hyperbilirubinemia (total bilirubin level, 5.1 mg per deciliter [87 μmol per liter]), a lactate dehydrogenase level of 8320 U per liter, and a negative Coombs' test. A peripheral-blood smear showed schistocytes (Panel A, arrows), spherocytes, and polychromasia suggestive of hemolytic anemia. Transesophageal echocardiography showed a jet of mild transvalvular mitral regurgitation (Panels B, C, and D, arrows; see the video) that immediately collided with the annuloplasty ring (Panels B, C, and D, arrowhead), redirecting the jet in an acute angle into the left atrium (Panel D, arrows). LA denotes left atrium, and LV left ventricle. Residual mitral regurgitation, even if mild, can result in erythrocyte fragmentation. The patient underwent mitral-valve replacement, which resulted in resolution of the hemolysis.
See that video please with the visit. https://t.me/drmohammedirfan
https://www.facebook.com/PrimalTRTOfficial/Women’s Reproductive Health & Daily WellnessFlexiLeafhttps://www.facebook.com/HumeHealthBodyPodOfficial/Pulsar Vexline Review 2026 - Legit Or Scam Trading Platform? Fact CheckGelatine Sculpt | Official WebsiteBurnSlim Official | Support Your Weight Management Journey
