



Massive Splenomegaly from Disseminated Mycobacterium avium–intracellulare Infection
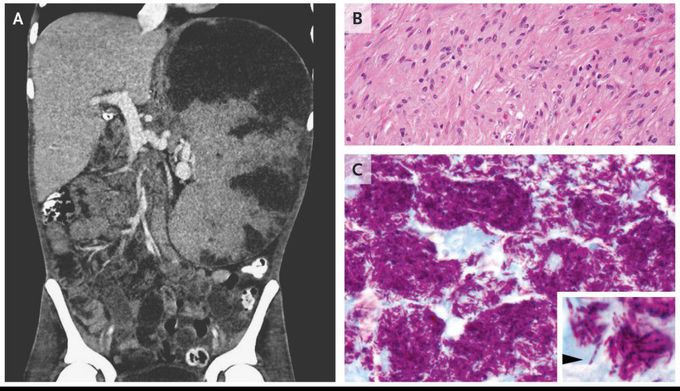
A 29-year-old man with perinatally acquired human immunodeficiency virus (HIV) infection presented to the hospital with abdominal pain and drenching night sweats. He had a history of intermittent adherence to antiretroviral therapy; on presentation, the CD4 count was 18 cells per cubic millimeter (reference range, 500 to 1500), and the HIV viral load was undetectable. Severe abdominal distention, splenomegaly, and diffuse abdominal tenderness to palpation were noted on physical examination. Computed tomography of the abdomen confirmed massive splenomegaly with multifocal infarction of the splenic parenchyma (Panel A). The patient underwent embolization of the splenic artery followed by splenectomy. Histopathological examination revealed near-total replacement of the splenic parenchyma by extensive necrosis and nodular aggregates of histiocytes with a spindle-shaped appearance (Panel B). Acid-fast staining revealed aggregates of mycobacteria that had undergone phagocytosis by histiocytes, a finding consistent with a phenomenon known as mycobacterial spindle-cell pseudotumor (Panel C, showing histiocytes with abundant intracellular mycobacteria; the inset, at higher magnification, shows a single intracellular mycobacterium [arrowhead]). Previously obtained blood cultures showed growth of Mycobacterium avium–intracellulare complex. Treatment with ethambutol, rifabutin, and clarithromycin was initiated, and the patient was discharged with a plan to continue long-term antimycobacterial therapy.

Living with HIV was one of the hardest experiences of my life. The fatigue, the emotional toll, and the uncertainty about the future weighed on me every single day. I had tried many treatments and medications, but nothing seemed to restore my health or energy the way I hoped.Out of both hope and desperation, I came across NaturePath Herbal Clinic. At first, I was skeptical but something about their natural approach and the powerful stories I read gave me the courage to try one more time.I began their herbal treatment program, and within a few weeks, I noticed small but meaningful changes more energy, better sleep, and a stronger immune system. Over the months, those improvements only grew. Today, I can truly say my life has changed. I feel healthier, more balanced, and finally in control of my well-being again.This isn’t just a testimony it’s a heartfelt recommendation to anyone living with HIV or any chronic condition. Don’t give up hope. I’m so grateful I gave NaturePath Herbal Clinic a chance. Visit their website to learn more: www.naturepathherbalclinic.com Email: info@naturepathherbalclinic.com
