



HIV Infection Manifesting as Proximal White Onychomycosis
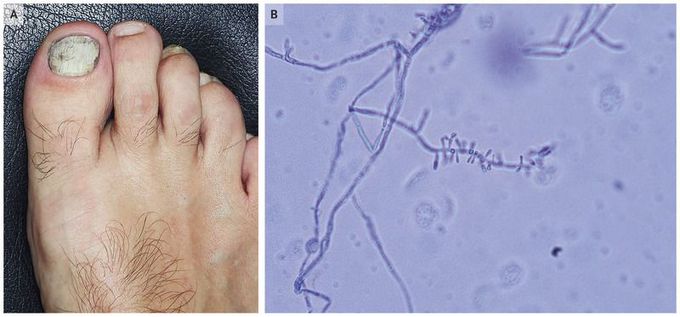
A 48-year-old-man presented to the dermatology clinic with a whitish discoloration and hyperkeratosis of the first toenail that had extended from the proximal to the distal nail during the past month (Panel A). The patient reported no history of trauma to the nail. He had no fever, weight loss, malaise, lymphadenopathy, or rash. Direct microscopic examination of superficial nail scrapings prepared with potassium hydroxide revealed numerous septate hyphae. Trichophyton rubrumwas isolated in a potato dextrose agar culture of the nail scrapings and had the characteristic red-wine color. Microscopic examination of the isolate stained with cotton blue revealed pyriform microconidia that had a “birds on a wire” appearance at the sides of the hyphae (Panel B). Although onychomycosis is a common fungal infection, it typically begins in the distal nail. Proximal white onychomycosis with rapid extension from the proximal to the distal nail is more unusual and can be suggestive of human immunodeficiency virus (HIV) infection or other conditions of immunocompromise. Serologic testing for HIV antibody was positive, with a viral load of 17,510 copies per milliliter and a CD4+ count of 40 cells per cubic millimeter. Treatment with antiretroviral therapy as well as antifungal therapy was initiated. At follow-up 9 months later, the patient had a good clinical response, with resolution of onychomycosis.

Living with HIV was one of the hardest experiences of my life. The fatigue, the emotional toll, and the uncertainty about the future weighed on me every single day. I had tried many treatments and medications, but nothing seemed to restore my health or energy the way I hoped.Out of both hope and desperation, I came across NaturePath Herbal Clinic. At first, I was skeptical but something about their natural approach and the powerful stories I read gave me the courage to try one more time.I began their herbal treatment program, and within a few weeks, I noticed small but meaningful changes more energy, better sleep, and a stronger immune system. Over the months, those improvements only grew. Today, I can truly say my life has changed. I feel healthier, more balanced, and finally in control of my well-being again.This isn’t just a testimony it’s a heartfelt recommendation to anyone living with HIV or any chronic condition. Don’t give up hope. I’m so grateful I gave NaturePath Herbal Clinic a chance. Visit their website to learn more: www.naturepathherbalclinic.com Email: info@naturepathherbalclinic.com
