



Lithium-Induced Nephropathy
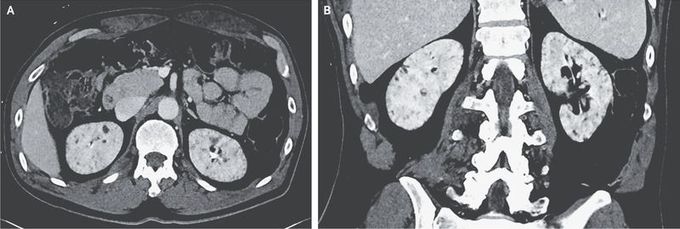
A 59-year-old man with a history of bipolar disorder was admitted to the hospital after a fall. He received a diagnosis of multiple fractures of the head and spine; the fractures were managed nonoperatively. During the hospitalization, his urine output was noted to range from 4 to 6 liters per day. The patient had taken lithium for 27 years before discontinuing the medication 8 years before the current presentation because of mild hyperparathyroidism and renal insufficiency (serum creatinine level, 1.5 mg per deciliter [130 μmol per liter]). While he was immobilized in the hospital, his serum sodium levels rose from 138 mmol per liter to 149 mmol per liter, with a urine osmolality that was inappropriately low (262 mOsm per kilogram). The urine osmolality did not increase with the administration of desmopressin, which confirmed a diagnosis of nephrogenic diabetes insipidus. As part of the evaluation for the fall, computed tomography of the abdomen and pelvis with contrast enhancement was performed, and the results showed numerous small renal cysts in the cortex and medulla of both kidneys (axial [Panel A] and coronal [Panel B] views, with a nonstandard window used to enhance visibility of cysts). Lithium is known to cause tubulointerstitial nephropathy, which may be seen on imaging as multiple small cysts. Management of this patient’s condition included a low-salt diet and a liberal intake of fluids. His sodium level normalized, and he was discharged to a rehabilitation facility.
