



Appendiceal Pinworms
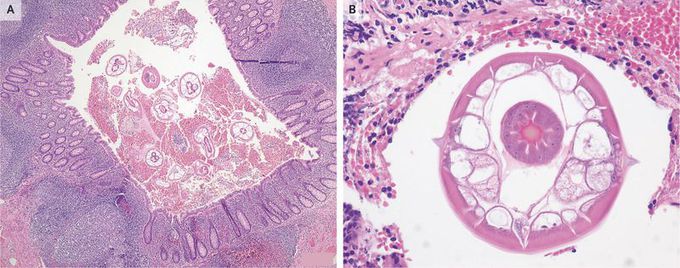
A 45-year-old man with a 1-day history of abdominal pain and loss of appetite presented to the emergency department. He did not have a fever. Physical examination revealed tenderness in the right lower quadrant of the abdomen. Rebound was present; Blumberg’s sign was negative. Laboratory results included a normal white-cell count, with 82% neutrophils. Abdominal ultrasonography was performed, but the results were inconclusive with regard to the presence or absence of appendiceal inflammation. An appendectomy was performed. The appendix was grossly normal, but pathological analysis revealed the presence of Enterobius vermicularis in the appendiceal lumen (Panels A and B, hematoxylin and eosin) and mild inflammation of the mucosa. E. vermicularis, known as pinworm, is a nematode that is most commonly found in young children, although adults can also be infected. The gravid female pinworm attaches to tissue near the cecum and migrates to the anus to deposit its eggs, which can cause perianal pruritus. Autoinfection and transmission occur through the ingestion of eggs from contaminated hands, bathroom fixtures, bedding, food, and other sources. It is difficult to determine definitively whether the presence of pinworm in the appendix was the cause of the patient’s presenting symptoms or was an incidental finding. After the appendectomy, the patient and his family were treated with mebendazole. At follow-up 6 months after surgery, the patient was asymptomatic.
