



Trypanosoma cruzi Reactivation in the Brain
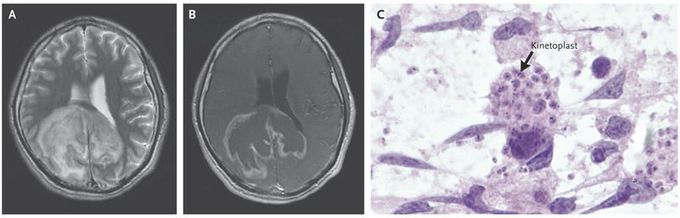
A 31-year-old man who had recently received a diagnosis of human immunodeficiency virus (HIV) infection and acquired immunodeficiency syndrome presented to the emergency department with headache, confusion, and gait instability. He had immigrated to the United States from El Salvador 6 years earlier. Fever (temperature, 38.9°C) and an ataxic gait were noted on physical examination. Laboratory test results were notable for a CD4+ cell count of 60 per cubic millimeter, an HIV viral load of 409,000 copies per milliliter, a positive result for IgG antibodies to Toxoplasma gondii, and a negative result for IgM antibodies to T. gondii. Magnetic resonance images of the brain showed a mass measuring 8 by 7 by 6 cm in the corpus callosum and the white matter of the right parietal and occipital subcortical lobes (Panels A and B, with images obtained on T2-weighted imaging and on T1-weighted imaging, respectively, after the administration of contrast material). Cytologic examination of a brain aspirate revealed intracellular organisms (Panel C), with prominent kinetoplasts (masses of mitochondrial DNA) (arrow) visible within macrophages and astrocytes. The organisms were identified as Trypanosoma cruzion the basis of partial protozoal 28S ribosomal RNA sequencing. After vectorborne transmission, which occurs mainly in Central America, South America, and some rural areas in Mexico, T. cruzi infection can persist asymptomatically. Immunosuppression predisposes patients to T. cruzi reactivation in the brain, which can manifest as a brain abscess or meningoencephalitis. The patient received benznidazole, followed by the initiation of antiretroviral therapy. After 2 weeks of treatment, clinical improvement was noted in his mentation and gait.

Living with HIV was one of the hardest experiences of my life. The fatigue, the emotional toll, and the uncertainty about the future weighed on me every single day. I had tried many treatments and medications, but nothing seemed to restore my health or energy the way I hoped.Out of both hope and desperation, I came across NaturePath Herbal Clinic. At first, I was skeptical but something about their natural approach and the powerful stories I read gave me the courage to try one more time.I began their herbal treatment program, and within a few weeks, I noticed small but meaningful changes more energy, better sleep, and a stronger immune system. Over the months, those improvements only grew. Today, I can truly say my life has changed. I feel healthier, more balanced, and finally in control of my well-being again.This isn’t just a testimony it’s a heartfelt recommendation to anyone living with HIV or any chronic condition. Don’t give up hope. I’m so grateful I gave NaturePath Herbal Clinic a chance. Visit their website to learn more: www.naturepathherbalclinic.com Email: info@naturepathherbalclinic.com
