



Disseminated Cutaneous Blastomycosis
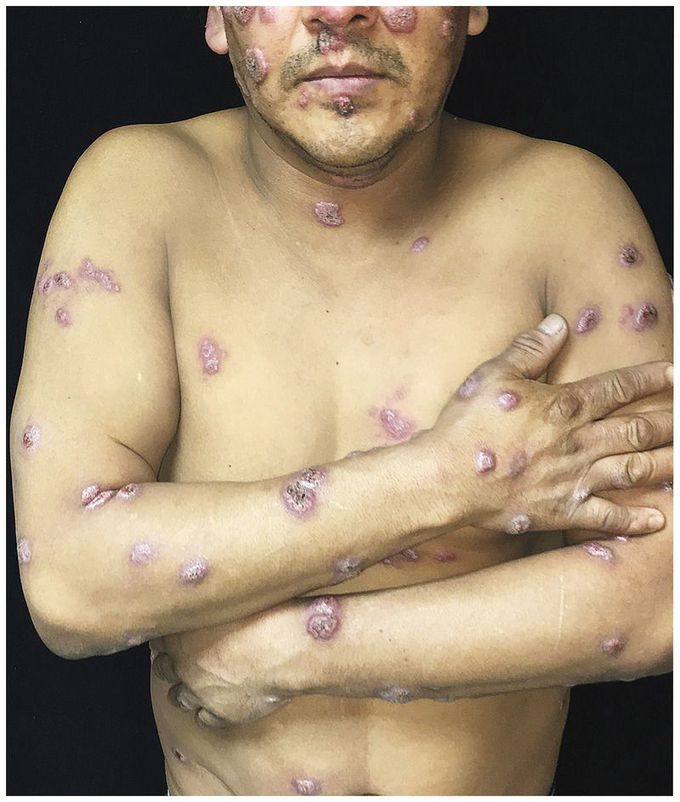
A 44-year-old man presented to the dermatology clinic with nonpruritic skin lesions over his body, including the face, chest, back, arms, and legs. Six months earlier, he had had fever, cough, and vomiting for 1 week. Subsequently, multiple nodules had appeared over his body. He worked in construction and reported no recent travel, exposure to pets, or contact with sick persons. A physical examination revealed numerous scattered crusted nodules and plaques that had indurated violaceous borders (shown). His lungs were clear to auscultation, and there was no notable lymphadenopathy. A radiograph of the chest did not show an infiltrate. The complete blood count was normal, and tests for human immunodeficiency virus infection and syphilis were negative. A fungal culture of skin tissue was negative; however, a skin biopsy showed pseudoepitheliomatous hyperplasia, intraepidermal neutrophilic abscesses, and round yeast forms with broad-based budding. Grocott methenamine–silver staining and mucicarmine staining confirmed a diagnosis of disseminated cutaneous blastomycosis, a pyogranulomatous fungal infection of Blastomyces dermatitidis or B. gilchristii. Patients may present with primary pulmonary infection or with disease that has spread hematogenously to the skin, bones, genitourinary tract, or central nervous system. This patient received treatment with itraconazole for 6 months; significant flattening of the lesions was observed at a follow-up visit 6 weeks after presentation.
