



Severe Mitral Stenosis
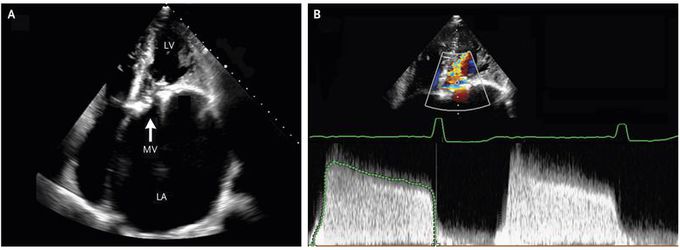
A 47-year-old man presented to the emergency department with a 6-month history of worsening exertional dyspnea. He had recently emigrated from Honduras and had a history of cardiac surgery as a child, but the initial diagnosis and specific procedure that had been performed were not known. The physical examination revealed a right parasternal heave, a loud S1, a midpeaking systolic ejection murmur (grade 2/6) at the upper sternal border, and a low-pitched diastolic rumble at the apex. An electrocardiogram showed atrial flutter with variable atrioventricular conduction. Transthoracic echocardiography revealed moderate aortic stenosis (calculated valve area, 1.3 cm2) and very severe mitral stenosis (calculated valve area, 0.5 cm2) ( Panel A; LA denotes left atrium, LV left ventricle, and MV mitral valve). The left atrium was enlarged, with an indexed atrial volume of 364 ml per square meter (normal value, <35). Color-flow Doppler images (Panel B, upper half) and a continuous-wave Doppler flow pattern (Panel B, lower half) showed the stenotic mitral valve during diastole. The continuous-wave Doppler flow pattern depicts flow velocity (vertical axis) and time (horizontal axis). The slow decline in transmitral flow velocity reflects the very slow decrease in left atrial pressure and slow increase in left ventricular diastolic pressure that occur in mitral stenosis. The mean transmitral gradient was 14 mm Hg (normal value, <3). The patient underwent replacement of the mitral and aortic valves with mechanical prostheses. At a 6-month follow-up visit, he had only slight limitations on physical activity (New York Heart Association class II).
