



Amebic Liver Abscess
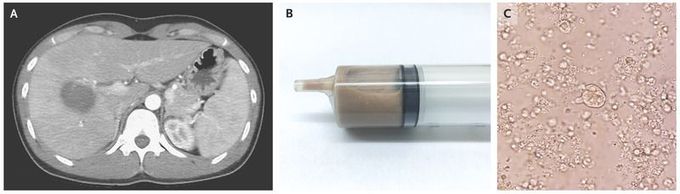
A 29-year-old man infected with the human immunodeficiency virus presented to the emergency department with a 2-day history of fever and pain in the right upper quadrant of the abdomen. His most recent CD4 cell count was 520 per microliter. Laboratory results showed an aspartate aminotransferase level of 208 IU per liter (reference range, 10 to 42), an alanine aminotransferase level of 467 IU per liter (reference range, 10 to 40), and a total bilirubin level of 2.4 mg per deciliter (reference range, 0.2 to 1.0). Computed tomography of the abdomen performed after the administration of contrast material revealed a ring-enhancing lesion in the liver that was suggestive of an abscess (Panel A). A reddish-brown material was obtained on percutaneous drainage of the abscess (Panel B). Microscopic examination revealed unicellular organisms with pseudopods (Panel C). An indirect hemagglutination test for antiamebic antibodies was positive, at a titer of 1:256. A polymerase-chain-reaction assay of stool confirmed infection with Entamoeba histolytica.E. histolytica infections result from the ingestion of amebic cysts. Contaminated food or water is typically the source. Metronidazole was administered for 2 weeks and was followed by 10 days of treatment with paromomycin to eliminate intracolonic cysts. The patient’s fever and abdominal pain subsided 2 days after the initiation of treatment, and the liver abscess had decreased in size on follow-up abdominal ultrasonography. At a 90-day follow-up visit, the patient had no further symptoms.
