



Parvovirus B19 Infection
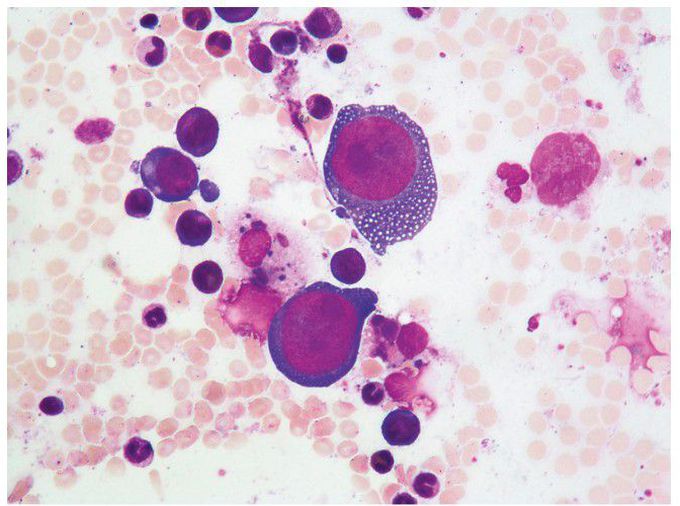
A 67-year-old woman presented to the emergency department with a 6-week history of progressive exertional dyspnea. Her medical history was notable for lung transplantation that had been performed 8 years earlier. Immunosuppressive medications included mycophenolate mofetil and tacrolimus. Laboratory studies showed normocytic anemia, with a hemoglobin level of 6.9 g per deciliter (reference range, 11.9 to 17.2). The hemoglobin level had been 12.7 g per deciliter 6 weeks earlier. White-cell and platelet counts were normal. The reticulocyte index was 0%, which aroused concern for red-cell aplasia or aplastic anemia. Bone marrow aspiration was performed and showed normal granulopoiesis and megakaryopoiesis, but reduced erythropoiesis. Giant proerythroblasts with basophilic and vacuolated cytoplasm, uncondensed chromatin, and large, intranuclear, purple-colored viral inclusions were present on the aspirate. These findings supported a diagnosis of parvovirus B19 infection, which was confirmed by polymerase-chain-reaction testing. The patient was treated with red-cell transfusions and intravenous immune globulin. By the time of hospital discharge, the hemoglobin level had increased, and at a 6-month follow-up, the anemia had completely resolved.
