



Coronary-Artery Occlusion from Kawasaki’s Disease
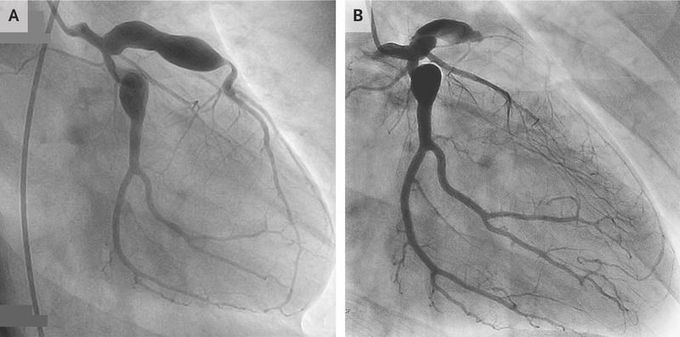
An 18-year-old man presented to the emergency department with chest pain. He had a history of Kawasaki’s disease, which had been diagnosed when he was 11 years of age. Despite treatment with intravenous immune globulin, coronary-artery aneurysms were detected on imaging (Panel A shows a coronary angiogram obtained 3 years before the current presentation). At the time of the current presentation, his medications included aspirin and warfarin. An electrocardiogram showed ST-segment elevations in leads V1 to V3. Emergency coronary angiography revealed occlusion of the left anterior descending artery (Panel B). Kawasaki’s disease is an acute, idiopathic, self-limiting vasculitis that primarily affects children. Clinical features include fever, nonexudative conjunctivitis in both eyes, mucositis, cervical lymphadenopathy, polymorphous rash, and changes in the hands and feet. Because not all these features are necessarily present and there is no specific diagnostic test for Kawasaki’s disease, the diagnosis may be missed in childhood or occur at such an early age that the adult patient has no recollection of illness. Affected children are at risk for cardiovascular complications. The patient underwent coronary-artery bypass surgery. At follow-up 3 years after presentation, he was doing well and had no further cardiac symptoms.
