



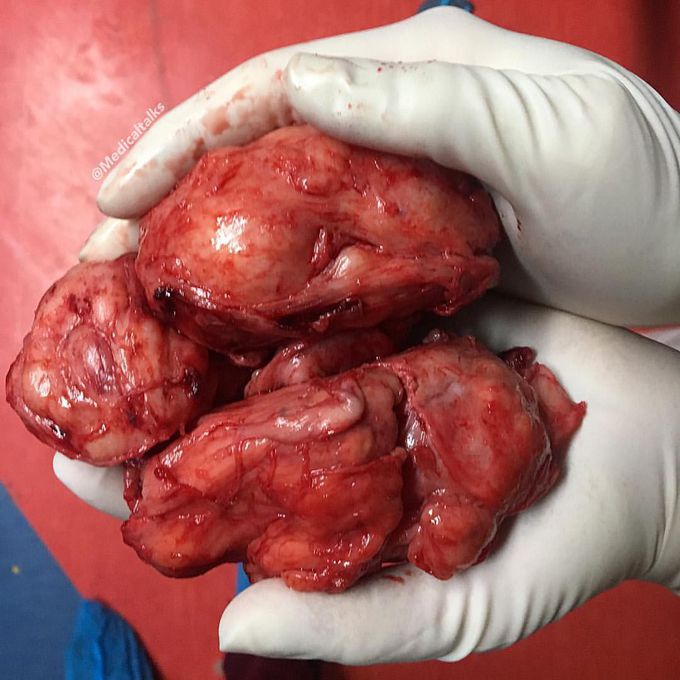
You’ve never seen a benign prostatic hyperplasia that big!!
By itself, benign prostatic hyperplasia or hypertrophy (BPH) implies the noncancerous increase in the size of the prostate gland, although rarely as big as seen here. Since there is actually an increase in the number of epithelial and stromal cells in the periurethral area of the prostate, not an enlargement of cells, the more accurate term is hyperplasia rather than hypertrophy. BPH is due to a combination of stromal and glandular hyperplasia, predominantly of the transition zone (as opposed to prostate cancer which typically originates in the peripheral zone). Androgens (Dihydrotestosterone and testosterone) are necessary for the development of BPH, but are not the direct cause for the hyperplasia. By the age of 60, 50% of men have BPH, and by 90 years of age the prevalence has increased to 90%. As such it is often thought of essentially as a 'normal' part of aging. Although a degree of prostatomegaly may be completely asymptomatic, the most common presentation is with lower urinary tract symptoms such as poor stream despite straining, hesitancy, frequency, incomplete emptying of the bladder, and nocturnal. Chronic bladder outlet obstruction secondary to BPH may lead to urinary retention, renal insufficiency, recurrent urinary tract infections, gross hematuria, and bladder calculi. All in all, surgical management for symptomatic patients is typically with a transurethral resection of the prostate. Early disease typically commences with finasteride (a 5-alpha-reductase inhibitor). Photo by @shelby_b_smith
Hemodynamic stimuli&nonhemodynamic stimuliEffects of sugar on teeth
