



Large-Bowel Obstruction from Hereditary Angioedema
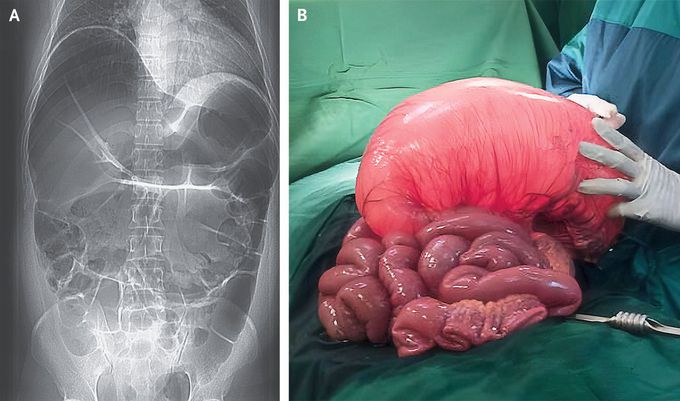
A 37-year-old man presented to the emergency department with an 8-hour history of severe abdominal pain and vomiting. An abdominal radiograph showed dilatation of the large bowel with prominent loops of small bowel (Panel A). Barium enema revealed high-grade obstruction at the splenic flexure. An emergency laparotomy was performed. The transverse colon was found to be massively dilated (Panel B) with severe mucosal edema that extended proximally to the ascending colon. A partial large-bowel resection was performed. After the procedure, the patient reported having had unexplained episodes of abdominal pain and swelling in his hands, feet, and scrotum, without associated hives or itching, since he was 18 years of age. He had never received treatment with an angiotensin-converting–enzyme inhibitor. He reported that his father and paternal relatives had also had similar episodes. Subsequent laboratory testing revealed a low C4 level and a C1 esterase inhibitor level of 6 mg per deciliter (reference range, 19 to 37). A final diagnosis of large-bowel obstruction from gut angioedema in the context of a delayed diagnosis of hereditary angioedema due to C1 esterase inhibitor deficiency was made. Long-term prophylactic treatment with danazol was prescribed, along with C1 esterase inhibitor replacement therapy for recurrent attacks of angioedema. In addition, the patient underwent genetic counseling for this autosomal dominant condition.
