



Cerebral Alveolar Echinococcosis
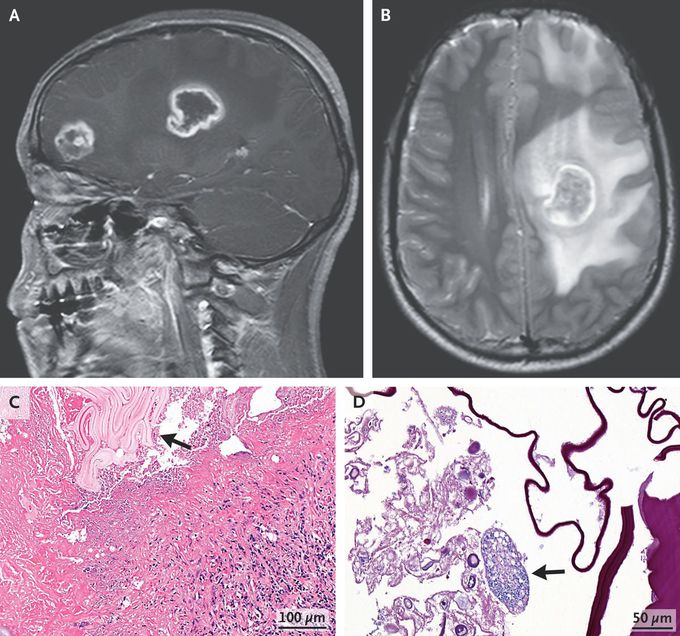
A 17-year-old boy presented to the emergency department with a 3-week history of dizziness, headache, and weakness of the right leg. Neurologic examination was notable for 4/5 strength in the right lower leg. Computed tomography (CT) of the head revealed ring-enhancing lesions in the frontal lobe and basal ganglia on the left side. Subsequent magnetic resonance imaging of the head also showed the lesions (Panel A; sagittal view, T1-weighted) as well as surrounding edema and midline shift (Panel B; axial view, T2-weighted). Testing for Echinococcus multilocularis and E. granulosus IgG antibodies was negative. Surgical excision of the lesions was performed. Histopathological testing showed necrotic tissue with surrounding granulomatous inflammation and an echinococcal laminated membrane (Panel C, arrow) as well an intact cyst (Panel D, arrow). A reverse-transcriptase–polymerase-chain-reaction assay identified E. multilocularis. CT imaging of the chest and abdomen did not show any other sites of disease. A diagnosis of primary cerebral alveolar echinococcosis was made. Alveolar echinococcosis is an invasive type of echinococcal infection that leads to tissue inflammation and destruction. The causative tapeworm is acquired by means of close contact with infected animals, which this patient had not reported. Postoperatively, a long course of albendazole was prescribed. At 2 months of follow-up, the patient’s symptoms had resolved.
