



Thrombectomy in Acute Ischemic Stroke
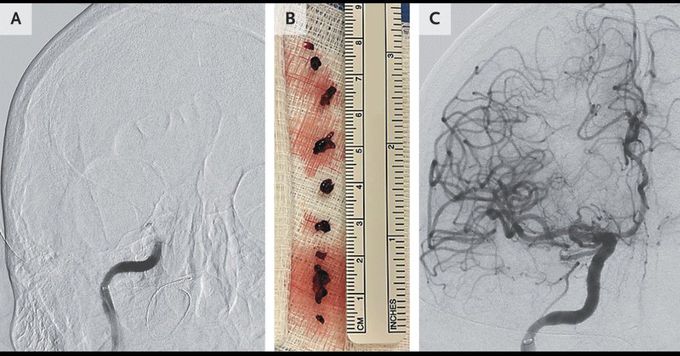
A 63-year-old man with atrial fibrillation, hypertension, and type 2 diabetes presented to the emergency department with weakness on the left side and difficulty speaking, both of which had begun 6 hours earlier. On examination, he had dysarthria, 0/5 strength in the left arm, and 1/5 strength in the left leg. Computed tomography (CT) of the head, performed without the administration of intravenous contrast material, showed no ischemic changes, but CT angiography of the neck revealed an occlusion of the right internal carotid artery. Intravenous thrombolysis was not performed; instead, endovascular therapy was initiated. Angiography, performed before the start of the intervention, confirmed a complete occlusion of the right internal carotid artery (Panel A). Mechanical thrombectomy, which was performed with the use of an aspiration catheter, resulted in the withdrawal of several large clot fragments (Panel B) and the restoration of perfusion (Panel C). The day after the procedure, atorvastatin and aspirin were administered, and 7 days after the procedure, the patient’s previous treatment with apixaban was resumed. In patients with acute ischemic stroke due to large-vessel occlusions, endovascular therapy improves neurologic outcomes in selected patients. At the time of hospital discharge 12 days after presentation, the patient’s neurologic examination was normal except for the strength in the left arm, which was assessed as 4/5.
