



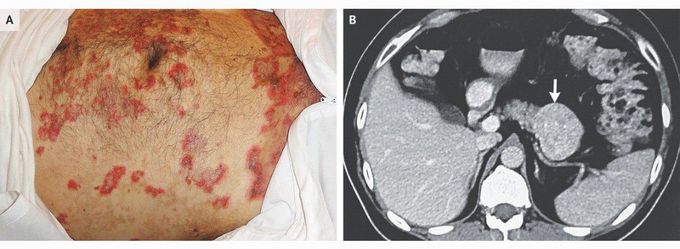
Necrolytic Migratory Erythema Associated with a Glucagonoma
A 48-year-old man presented to the dermatology clinic with a 2-month history of an itchy rash that had started in the genital region and had progressed to involve the torso, hands, and legs. He had recently received a diagnosis of diabetes mellitus and also reported a 13-kg weight loss since receiving that diagnosis. On examination, erythematous patches and plaques at various stages of healing were seen (Panel A). Biopsy revealed ballooning of the upper spinous keratinocytes with a thick crust of necrotic debris. This appearance was consistent with necrolytic migratory erythema, and an underlying glucagonoma was suspected. Serum glucagon levels were elevated, and a computed tomographic scan of the abdomen showed an exophytic hypervascular mass in the pancreatic tail with focal calcification (Panel B, arrow). A distal pancreatectomy was performed, and pathological examination confirmed the diagnosis of a glucagonoma. The rash began to abate soon after surgery and had completely resolved at follow-up 3 months later. At 5 years of follow-up, there had been no recurrence of the rash or glucagonoma.
To all you who might know this fisease and clinical dermatological manifestations, is there a reason why the rash started in the genital region?
