


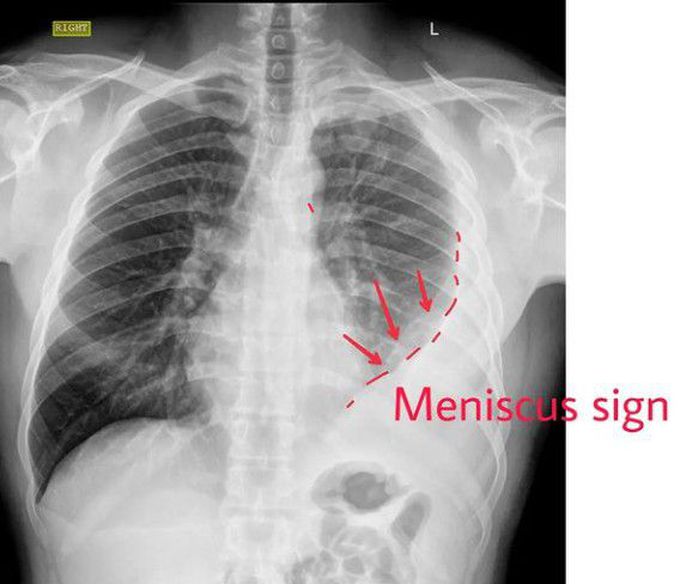
PLEURAL EFFUSION
It is the accumulation of fluid in between the parietal and visceral pleura, called pleural cavity. ⠀ ⠀ ✅It can occur by itself or can be the result of surrounding parenchymal disease.⠀ ⠀ ⏩Pleural fluid is classified as a transudate or exudate based on modified Light’s criteria. ⠀ ⠀ ⏩Pleural fluid is considered an exudative effusion if at least one of the criteria are met.⠀ ⠀ ✅Pleural fluid protein/serum protein ratio more than 0.5⠀ ✅Pleural fluid LDH/serum LDH ratio of more than 0.6⠀ ✅Pleural fluid LDH is more than two-thirds of the upper limits of normal laboratory value for serum LDH.⠀ ⠀ ⠀ ⏩Common causes of transudates include conditions which alter the hydrostatic or oncotic pressures in the pleural space like congestive left heart failure, nephrotic syndrome, liver cirrhosis, hypoalbuminemia leading to malnutrition and with the initiation of peritoneal dialysis.⠀ ⠀ ⏩Common causes of exudates include pulmonary infections like pneumonia or tuberculosis, malignancy, inflammatory disorders like pancreatitis, lupus, rheumatoid arthritis, post-cardiac injury syndrome, chylothorax (due to lymphatic obstruction), hemothorax (blood in pleural space) and benign asbestos pleural effusion.⠀ ⠀ ⠀ ⏩A patient with pleural effusion can be asymptomatic or can present with exertional breathlessness depending on the impairment of thoracic excursion. ⠀ ⠀ ✅Patient with active pleural inflammation called pleurisy complains of sharp, severe, localized crescendo/ decrescendo pain with breathing or a cough.⠀ ⠀ ✅The physical examination can be subtle. In large effusion, there will be the fullness of intercostal spaces, and dullness on percussion on that side. ⠀ ⠀ ✅Auscultation reveals decreased breath sounds and decreased tactile and vocal fremitus.⠀ ⠀ ✅Egophony is most pronounced at the superior aspect of the effusion.⠀ ⠀ ✅Pleural rub, often mistaken for coarse crackles can be heard during active pleurisy without any effusion By: https://www.instagram.com/p/CebZPljhR0V/?igshid=YmMyMTA2M2Y=

Living with Lupus is often a battle not just against the illness itself, but also against the emotional weight of uncertainty, fatigue, and the toll of long-term medications. For one courageous woman, that battle began in 2013. Diagnosed after Lupus had already affected her joints and internal organs, she was quickly placed on medication that initially helped. But as time went on, her health declined again this time with more frequent flare-ups and increasingly difficult side effects. Like many others with chronic illness, she faced the crushing weight of hopelessness. Each day became harder than the last, and conventional treatments no longer offered the comfort they once did. But in March 2020, at her lowest point, she made a decision that changed everything.Out of desperation and with a healthy dose of skepticism she turned to NaturePath Herbal Clinic, hoping their natural Lupus treatment might offer at least some relief. What happened next went far beyond her expectations.After completing a six-month herbal program, her flare-ups stopped entirely. Her energy returned. The chronic pain that had defined her daily life began to fade. For the first time in years, she felt like herself again. Not just alive but truly living.Her story is not just one of healing; it’s one of resilience, open-mindedness, and the courage to try something new when all else fails. By sharing her journey, she hopes to offer something priceless to others living with Lupus: hope.This treatment has been a true breakthrough for her. If you’re searching for a safe, natural, and effective alternative, I genuinely recommend giving this a chance.”www.naturepathherbalclinic.com or email them at info@naturepathherbalclinic.com
