



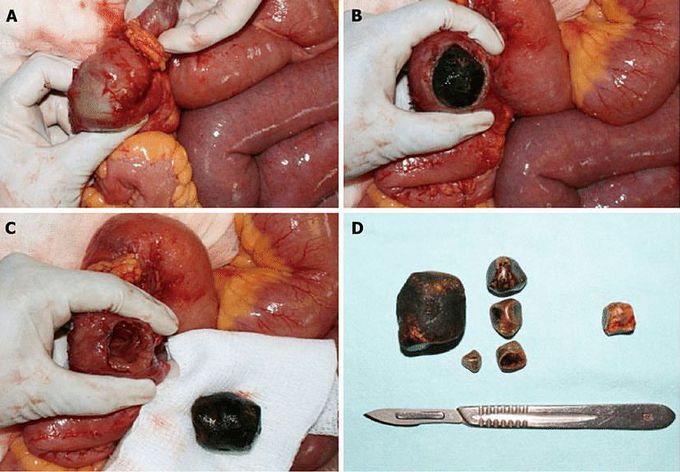
Gallstone extracted from the bowel!
Gallstone ileus occurs when a gallstone passes through a billiary-enteric fistula into the small bowel. As the stone advances it may cause intermittent “tumbling” obstruction with diffuse abdominal colicky pain and vomiting until finals lodging in the ileum, the narrowest section of the bowels, several days later. This image shows the surgical findings in a patient with gallstone ileus. A: An impacted gallstone was found in distal jejunum. A smaller gallstone proximal to the impacted one is observed; B: Enterotomy over the site of the impacted gallstone; C: Intestinal wall compromise due to gallstone impaction can be observed; D: The offending gallstone, plus four of smaller dimensions found in proximal jejunum. An obstructing gallstone was found and extracted from the common bile duct in the same patient (gallstone on the right). Enterolithotomy is the most commonly surgical procedure performed. Through an exploratory laparotomy, the site of gastrointestinal obstruction is localized. A longitudinal incision is made on the anti mesenteric border proximal to the site of gallstone impaction. When possible, through gentle mani pulation the gallstone is brought proximally to a non edematous segment of bowel. Most of the times, this is not possible due to the grade of impaction of the gallstone. The enterotomy is performed over the gallstone and it is extracted. Careful closure of the enterotomy is needed to avoid narrowing of the intestinal lumen and a transverse closure is recommended. Bowel resection is sometimes necessary, particularly in the presence of ischemia, perforation or an underlying stenosis. Manual propulsion of the gallstone through the ileocecal valve should be reserved for highly selected situations because of danger of mucosal injury and bowel perforation. Similarly, attempts to crush the gallstone in situ can damage the bowel wall and should be avoided. Multiple gallstones can generally be extracted through a single incision by clearing the gut and moving smaller gallstones towards bigger ones.
Hemodynamic stimuli&nonhemodynamic stimuliEffects of sugar on teeth
