



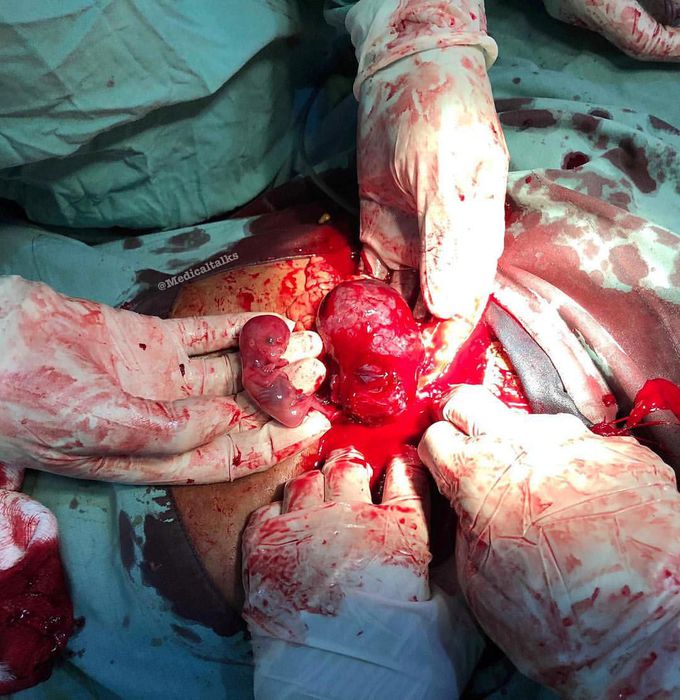
A post-laparoscopic picture of a tubal gestation that had been teased out after linear salpingostomy!!
Ectopic pregnancy occurs when a blastocyst implants in an extrauterine location such as the fallopian tube, which is uninhabitable for proper fetal growth. This 32 years old was admitted to hospital after 11 weeks of missed menstrual period (amenorrhea) and presented with severe right iliac fossa pain and vaginal bleeding, associated with dark yellow spotting. The pain was tolerated and the symptoms resolved the same day. No bleeding, clots or meaty tissue were noted. On examination, she had abdominal tenderness and cervical motion tenderness. The patient complained of sudden onset of right lower quadrant tenderness. The pain was characterized as squeezing, rated as 10/10 on the pain scale. No medications were taken to relieve the pain. Persistence of above symptoms prompted her to seek consultation. Her past medical history was a previous tubal surgery of ectopic pregnancy, which is an alarming risk factor. The diagnosis of ectopic pregnancy was made by pregnancy test (positive hCG) and transvaginal ultrasound, which confirmed the gestational sac was seen at an ectopic site, most commonly the fallopian tube. The patient was at risk for an intra-abdominal pain due to ruptured ectopic pregnancy. Blood in the abdomen and pelvis produces irritation of the nearby structures and can cause diffuse abdominal pain and cervical motion tenderness. Laparoscopic surgery was done to gain access to the pelvis, incise the affected tube and remove the fetus (salpingostomy). In more severe cases surgeons remove the affected tube with the pregnancy (total salpingectomy). Phot by @marty_mohamed
Hemodynamic stimuli&nonhemodynamic stimuliEffects of sugar on teeth
