


Answer please
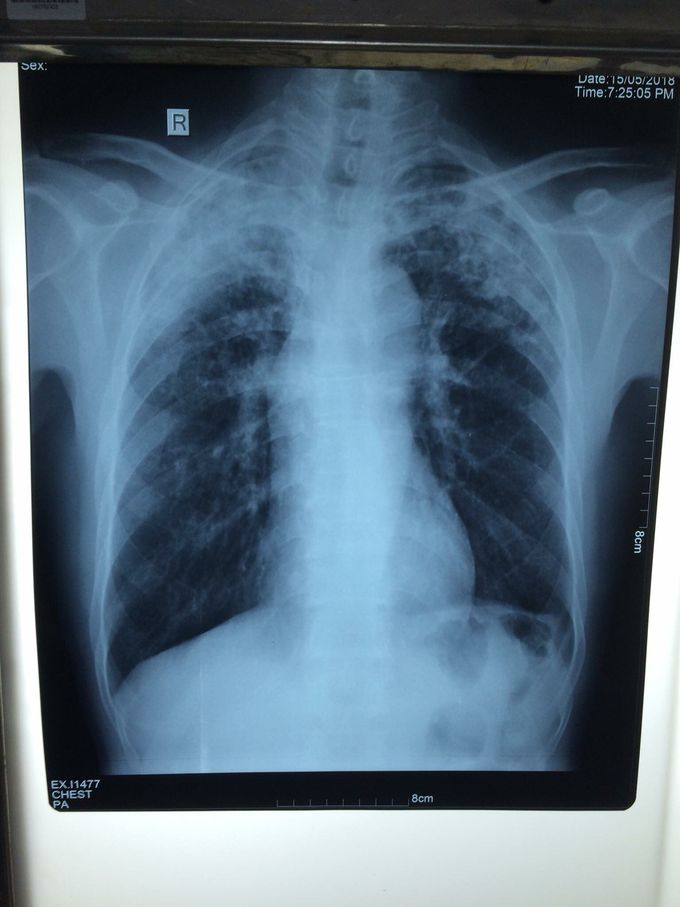
case report from Pneumo Department KSFH, Patient 50 years old (Male) Cc: Dyspnea associate with chronic productive cough and oppression thoracic. Past history: -Non previous anti-TB treatment -Non TB disease -Primary smoking 25 packing per year -DM and HTN Unknown PE report -Crackle sound bilateral on upper lobe -Tachycardia -Hemodynamic stable -Dyspnea type polypnea RR >26 with SpO2: 92% air environmental -Other system normal Questions 1. Depend on imageries include CxR, ECG and Clinical symptoms and PE. what's your 1st Dx...? 2. Next step to confirm Dx base on CxR link to your clinical Dx....? 3. Management process...? 4. If condition not improve, alteration on GA and Perisistent fever. Next step to do....? 5. If condition of patient developing to severe sepsis. What's your essential process and best way to solve Pt....? 6. Which of Bilan do you need to evaluation and observes evolution of the disease....? 7. Indication of Bilan control....?
1. Susp. TB, 2. Sputum tes 3. Nebulizer with short beta2agonis, 4. Intravenous fluid with Nacl 0,9%+Aminofilin drip, 5. Antibiotik injection such as ceftriaxone, 6. ? 7. ?

1. Susp TB, especially if there is any TB’s pulmo and systematic symptoms. 2. Sputum BTA, take tuberculin test in children can be helpful than sputum test. 3. O2, Nebu, ambroxol 4. Wide spectrum Antibiotics to prevent sepsis anf if the px not improve 5.&6. Its hard to decide any management if havent see the condition directly
https://www.facebook.com/AspenDoseCBDGummiesPage/
