



Respiratory Diphtheria
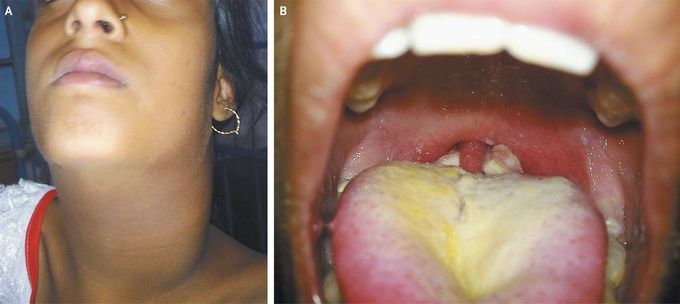
A 13-year-old girl with a history of incomplete childhood immunization (she had received only the first of three doses of the diphtheria–pertussis–tetanus vaccine), residing in West Bengal, India, presented to the emergency department of the Infectious Diseases Hospital in Kolkata in June (during the rainy season of June through September). She had had a fever, severe sore throat, bull neck (Panel A), hoarse voice, and respiratory distress for 8 days. She appeared sick, had tachycardia with normal blood pressure, and had bilateral, yellowish white pharyngeal patches with congestion (Panel B). Bleeding was observed on an attempt to dislodge a patch during collection of a throat-swab specimen for culture. She received a clinical diagnosis of diphtheria. Treatment was initiated immediately (80,000 IU of antidiphtheria serum administered as a slow intravenous infusion [a skin hypersensitivity test was negative] and penicillin G procaine at a dose of 600,000 units given intramuscularly every 12 hours for 10 days until the patient could swallow, followed by penicillin V at a dose of 250 mg given orally four times daily for another 4 days). The throat culture was positive for Corynebacterium diphtheriae. The patient recovered without any major complication, with the bull neck disappearing within 1 week after the initiation of treatment. Diphtheria is endemic in India, and no similar cases were reported from the same district of West Bengal during the same period. Alakes K. Kole, M.D. Rammohan Roy, M.D. Infectious Diseases Hospital, Kolkata, West Bengal, India source: nejm.org

