



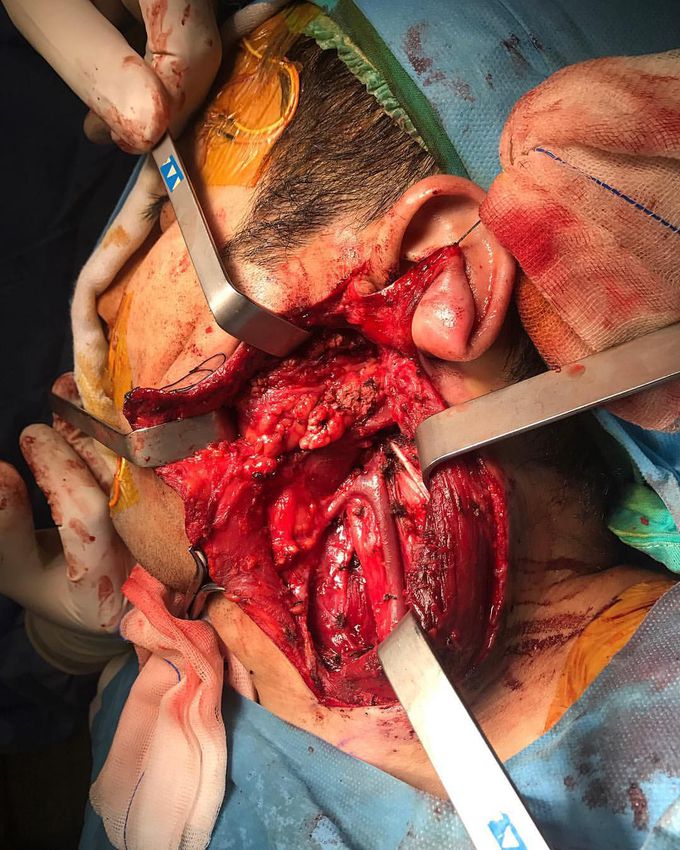
Parotidectomy for a pleomorphic adenoma tumor in the parotid gland!
This young man had a slow growing and multiple nodular mass on the left side of his face. There were no signs of pain, tenderness or paresthesia, as well as no sign of infection in needle aspiration. After performing FNA (fine-needle aspiration biopsy), the mass has been diagnosed as a pleomorphic adenoma, a benign and common salivary gland neoplasm, characterised by neoplastic proliferation of parenchymatous glandular cells along with myoepithelial components. The surgical treatment was a superficial parotidectomy with preservation of the facial nerve. Most of the salivary gland tumors occur in the parotid and are benign. The most common type is a pleomorphic adenoma (mixed tumor). Malignant transformation is possible, resulting in carcinoma ex pleomorphic adenoma, but this usually occurs only after the benign tumor has been present for 15 to 20 years. If malignant transformation occurs, the cure rates are very low, despite adequate surgery and adjuvant therapy. Other benign tumors include monomorphic adenoma, oncocytoma, and papillary cystadenoma. These tumors rarely recur and rarely become malignant. The photograph shows the jugular vein at the center, the acoustic nerve below, and the facial nerve to the right. The facial nerve normally courses and divides within the core of the parotid gland. Any surgical procedure involving the parotid gland (parotidectomy for a benign tumor) requires precise identification and preservation of the facial nerve fibers. This nerve not only carries nerve impulses to the muscles of the face, but also to the tear glands, to the saliva glands, and to the muscle of the stirrup bone in the middle ear (the stapes). It also transmits taste from the front of the tongue. Since the function of the facial nerve is so complex, many symptoms may occur when the fibers of the facial nerve are disrupted. Photo credit @mhmtschahtuer
Hemodynamic stimuli&nonhemodynamic stimuliEffects of sugar on teeth
