



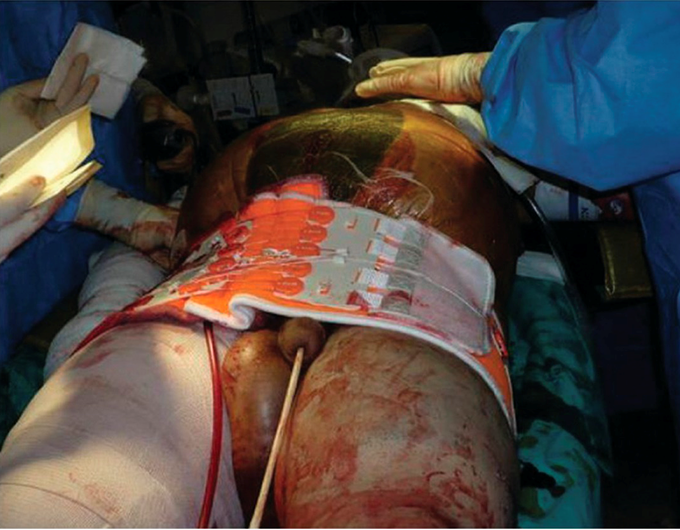
Pelvic Fracture Secondary to High-Energy RTA: Initial Management
Pelvic fracture, and consequent hemorrhage is one of the most common cause of morbidity in isolated pelvic fractures and polytrauma patients. According to statistics, 7.3% patients with pelvic fractures associated with high-energy RTA do not survive during hospital stay; 14.2% patients die within 3 months due to late complications. The National Institute for Health and Care Excellence (NICE) and British Orthopaedic Association (BOA) have devised guidelines for management of pelvic fractures. The goal is increased survival of the patient and minimizing risk of associated complications. Preliminary management follows Advanced Trauma Life Support (ATLS) ABCDE protocol in general hospital. Transfer to major trauma center is imperative in case of hemodynamic instability and polytrauma. Pelvic binder should be applied to stabilize the fracture. In case of open fracture, administer IV prophylactic broad-spectrum antibiotics within one hour of hospital admission. First-line analgesic in case of polytrauma or high-energy RTA-associated pelvic fracture is morphine, given intravenously. Tranexamic acid can be given to reduce blood loss. Contrary to low-energy pelvic fracture, where AP pelvic radiography is sufficient for complete diagnosis, contrast-enhanced CT scan of head, abdomen and pelvis is particularly important in high-energy RTA. BOA also suggest head to toe imaging. Active arterial bleed, if uncontrolled, should be stopped invasively through pelvic packing. If no laparotomy is required, selective embolization of arteries done by interventional radiologist should cease the hemorrhage. Pelvic binder should be removed within 24 hours to prevent pressure sores. In case of isolated pelvic trauma, pelvic surgeon should be called. In case of polytrauma, a multidisciplinary team should be taken on board. Furthermore, all the associated complications like urological injuries, colorectal injuries, and nerve injuries should be assessed by respective specialists. Once the initial management is done and the patient is hemodynamically stabilized, orthopaedic procedures should be performed to reduce fractures. Source An overview of the key principles and guidelines in the management of pelvic fractures https://journals.sagepub.com/doi/full/10.1177/1750458920947358 Image taken from Atlas of Surgical Techniques in Trauma https://www.cambridge.org/core/books/atlas-of-surgical-techniques-in-trauma/pelvic-fractures-and-bleeding/2F9E893EE6EF881B4B4EB05C88CDCC92
Wow! By the statistics I shouldn't even be here. Was riding a motorcycle when I was t-boned by an SUV going over 70mph. My right hip was demolished. This was 16 years ago and the damn thing still has a non-union fracture at the right inferior pubic ramus. There was an ORIF that spans from the left side of the pubic tubercle around the outer edge all the way to the spinal column. ORIF to reattach the pelvis to the spinal column. Destruction of the last two bones in my coccyx. Hip was dislocated and had a fracture of the greater trochanter of the femur with several other femur fractures, along with many, many other fractures of the tibia, fibula, tibial plateau, ankle and bones in my foot that ultimately led to an AKA s/p eight years.
woahh! your journey sounds miraculous. hope you're doing all okay now. take care!
Hemodynamic stimuli&nonhemodynamic stimuliWhat is Rheumatoid Arthritis? | Johns Hopkins RheumatologyAnkylosing Spondylitis | HLA-B27, Pathophysiology, Signs & Symptoms, Diagnosis, TreatmentWhat is scoliosis?Osteosarcoma - Pathology, Symptoms, Diagnosis, TreatmentEffects of sugar on teethExternal nose bones
