



Cerebral Metastases
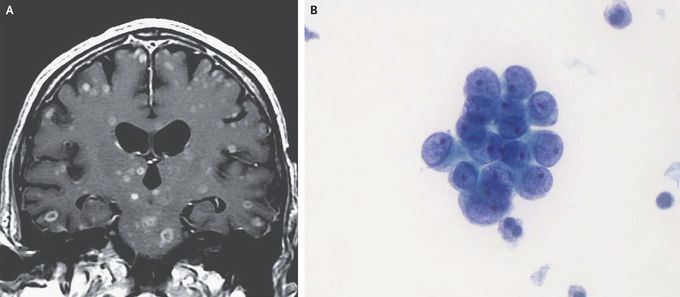
A 71-year-old man was transferred to our hospital with altered mental status that had progressed over the preceding 3 weeks. One month before presentation, he had presented to his primary care physician with abdominal pain and anemia. A colonoscopy revealed an obstructing, circumferential mass in the right colon, and findings on biopsy were consistent with adenocarcinoma. Computed tomography of the chest, abdomen, and pelvis revealed wide-spread metastases, including a lesion in the lower lobe of the right lung and multiple skeletal lesions in addition to the mass in the right colon. Surgical resection of the colonic mass was performed, and findings on pathological assessment confirmed a diagnosis of adenocarcinoma. Given the recent change in the patient’s mental status, gadolinium-enhanced magnetic resonance imaging of the head was performed and revealed numerous lesions, some with ring enhancement, but without substantial edema or mass effect (Panel A). Cerebral metastases were considered to be the most likely explanation, but the differential diagnosis of the brain lesions also included bacterial abscesses, neurocysticercosis, and tuberculosis. Blood cultures and evaluations for the human immunodeficiency virus and tuberculosis were negative. A lumbar puncture was performed, and cytologic analysis of the cerebrospinal fluid showed clusters of adenocarcinoma cells (Panel B). The patient’s family decided to pursue palliative care, and the patient died 1 week later.
