



Idiopathic Aqueductal Stenosis
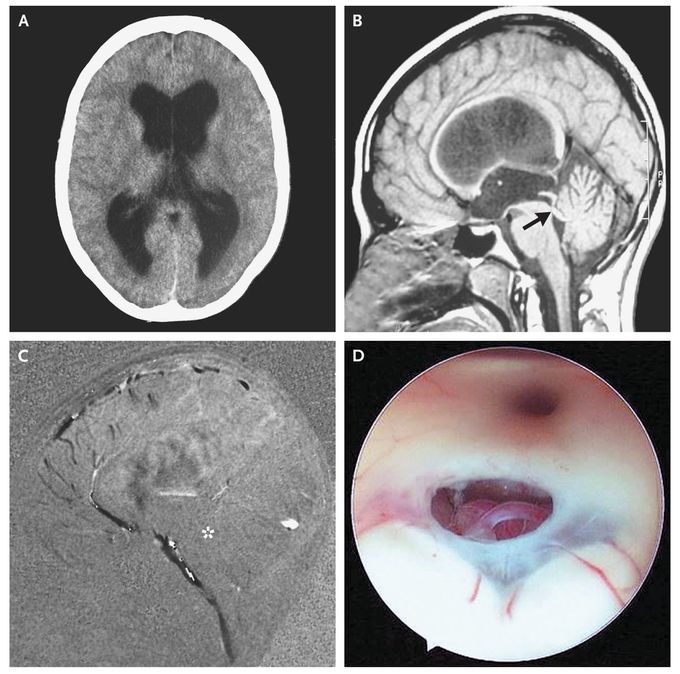
A 21-year-old woman presented with somnolence and confusion. She reported having progressively worsening headaches, nausea, and vomiting over the previous 5 months. Funduscopic examination showed bilateral papilledema as a clinical sign of intracranial hypertension. Computed tomography (Panel A) and magnetic resonance imaging (MRI) showed supratentorial hydrocephalus due to aqueductal stenosis (Panel B, arrow). Sagittal cine-phase MRI with the administration of contrast material showed a lack of flow-signal intensity at the aqueduct level (Panel C, asterisk). The patient received a diagnosis of idiopathic aqueductal stenosis, the most common form of obstructive hydrocephalus in adults. There was no evidence of a secondary cause of aqueductal stenosis, such as a tumor, infectious ventriculitis, or intraventricular hemorrhage. An endoscopic ventriculostomy was performed (Panel D) (see videos) by opening the floor of the third ventricle into the subarachnoid space of the brain-stem cisterns. This procedure treats idiopathic aqueductal stenosis by restoring the circulation of cerebrospinal fluid, without the need for an external ventriculostomy or ventriculoperitoneal shunt. There were no complications, such as meningitis, severe bleeding, new onset of neurologic deficits, leak of cerebrospinal fluid, or pneumocephalus. The patient had a good response to the procedure, with complete neurologic recovery. Five years later, she remained asymptomatic, and MRI showed no recurrence of hydrocephalus.
See that video please with the visit. https://t.me/drmohammedirfan

