



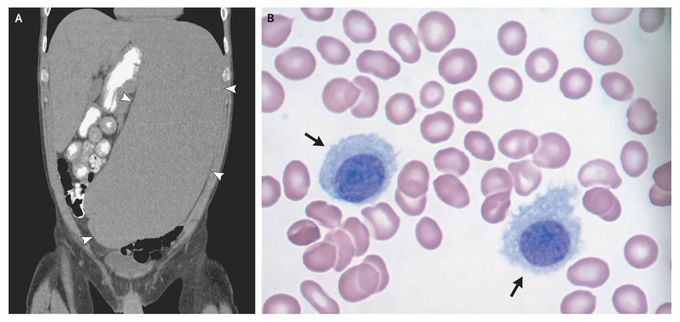
Massive Splenomegaly in Hairy-Cell Leukemia
A 63-year-old man presented with a 6-month history of fatigue, weight loss, and gingival bleeding. Physical examination suggested the presence of a massively enlarged spleen, a finding confirmed on a reconstructed coronal computed tomographic image of the abdomen (Panel A, arrowheads). A complete blood count revealed thrombocytopenia (platelet count, 27,000 per microliter; reference range, 150,000 to 400,000) and lymphocytosis (lymphocyte count, 8900 per microliter; reference range, 1000 to 4800). Microscopical examination of a bone marrow aspirate revealed abnormal lymphocytes with abundant light-blue cytoplasm, round nuclei, fine chromatin, and irregular projections of the cell membrane (Panel B, arrows). Similarly abnormal lymphocytes were also evident on microscopical examination of a peripheral-blood smear. Immunohistochemical staining was positive for tartrate-resistant acid phosphatase. Immunophenotyping by means of flow cytometry was positive for CD19, CD20, CD11c, CD25, and CD103 and negative for CD5 and CD10. These findings confirmed a diagnosis of hairy-cell leukemia. Named for the microscopical appearance of its malignant cells, this uncommon, indolent B-cell non-Hodgkin's lymphoma often presents with cytopenias, systemic symptoms, and massive splenomegaly. This patient had a complete remission after treatment with the purine analogue cladribine. He remained in remission at his last follow-up, at 9 months, with normal peripheral-blood counts, a normal bone marrow aspirate, and no evidence of splenomegaly.
These pictures are incredible showing the hairy cell cytoplasm wall. His medical team, With their excellent treatments, placed this patient into remission. Thank you Dr. Sheikh for sharing
