



Subungual Tumor of the Thumb
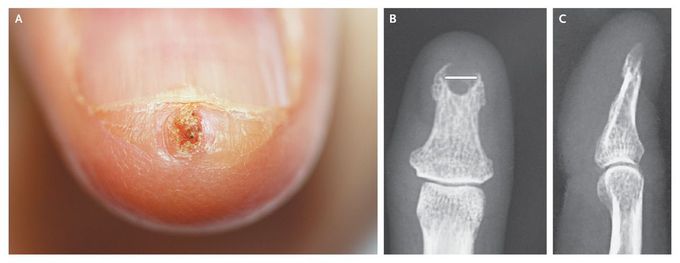
A 40-year-old woman presented with a 3-month history of a painful subungual mass of the left thumb. Examination revealed a tender, keratotic, subungual nodule (Panel A). Radiography of the digit showed a well-defined, cup-shaped erosion of the distal phalanx corresponding to the overlying subungual nodule (Panels B and C; the scale bar in the lesion in Panel B indicates 5 mm). There was no periosteal reaction. A wide excision was performed. Histologic examination showed the appearance of subungual keratoacanthoma. Solitary distal digital keratoacanthoma is a rare, usually painful, and destructive variant of keratoacanthoma. It may be locally aggressive, appearing as a crescent-shaped soft-tissue mass with an osteolytic defect of the underlying bone. Histologic features are usually indistinguishable from those of squamous-cell carcinoma. Immunohistochemical staining with Ki67, a marker of proliferation, may be helpful, but the diagnosis is based mainly on the natural history. This fingertip lesion characterized by eroding bone should be differentiated from other bone tumors such as osteosarcoma. At follow-up 6 months later, the patient had no pain and there was no recurrence.

Cratocanthoma is non melanotic tumor of skin. Usually its benign but have potentially to be malignant. Good presentation nice work.
At first glance I am thinking of glomus tumour as the presentation and history pain mimic to it. Ultimately, histopathology is let us know the diagnosis
