



Osteitis Fibrosa Cystica
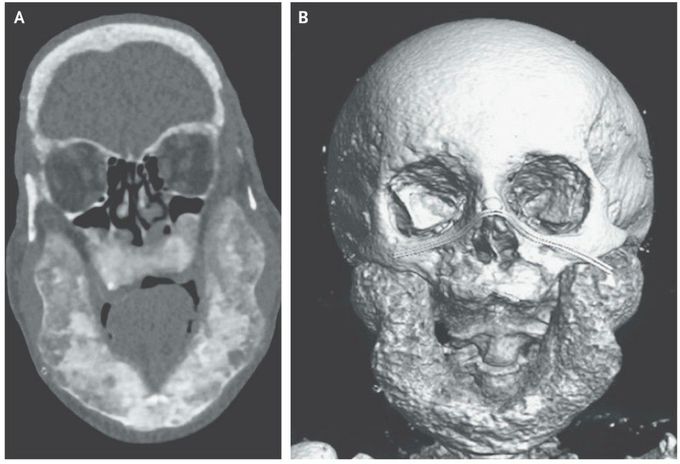
A 48-year-old man who had recently immigrated to France and had not yet established routine medical care presented to the emergency department with shortness of breath. He had a history of end-stage renal disease for which hemodialysis had been initiated 10 years earlier. A physical examination showed mandibular prominence, thoracic kyphosis, and crackles in both lungs. Laboratory studies showed a calcium level of 1.9 mmol per liter (7.6 mg per deciliter) (normal range, 2.2 to 2.6 mmol per liter [8.8 to 10.4 mg per deciliter]), a phosphate level of 0.96 mmol per liter (2.97 mg per deciliter) (normal range, 0.81 to 1.58 mmol per liter [2.51 to 4.89 mg per deciliter]), a 25-hydroxyvitamin D level of 13 nmol per liter (5.2 ng per milliliter) (normal range, 75 to 175 nmol per liter [30 to 70 ng per milliliter]), and a parathyroid hormone level of 4081 ng per liter (normal range, 11.5 to 78.4). Computed tomography (Panel A) and three-dimensional reconstruction (Panel B) of the face revealed mandibular hypertrophy and a heterogeneous appearance of the bone, with both cystic lesions and patches of osteolysis. Similar bony lesions were found in the spine, iliac bone, and femur. Osteitis fibrosa cystica is a skeletal disorder that is caused by sustained hyperparathyroidism, often due to chronic renal failure, resulting in the formation of cystlike tumors in the bone. Treatment with cinacalcet and vitamin D supplementation were started. His shortness of breath resolved after hemodialysis was reinitiated. At a follow-up visit 6 months after treatment was initiated, the parathyroid hormone level had decreased to 1743 ng per liter and the 25-hydroxyvitamin D level had returned to a normal level, but the bone lesions had not regressed

