



Nasal Deformity in Granulomatosis with Polyangiitis
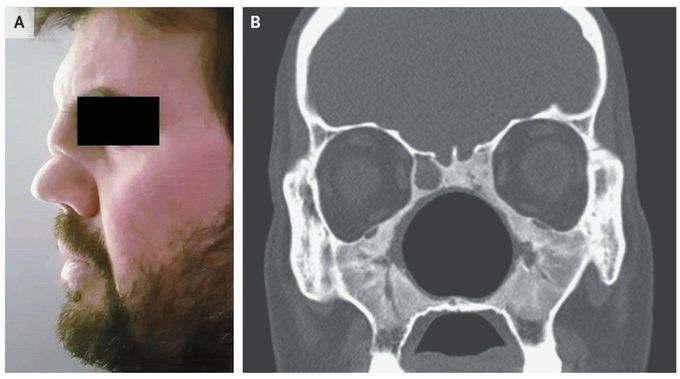
A 42-year-old man who had received multiple treatments for rhinosinusitis over the preceding 4 years presented to the clinic with a 3-month history of worsening cough, shortness of breath, and fever. He had no history of cocaine use. Physical examination showed a saddle-nose deformity (Panel A) with inflamed nasal mucosa and nasal crusting. Auscultation of the lungs was notable for wheezes and rales in both lungs. A computed tomographic (CT) scan of the chest showed multiple pulmonary nodules, and a CT scan of the face showed extensive destruction of the structural bones of the midface that had resulted in the formation of a large nasal cavity (Panel B). Testing for proteinase 3 antineutrophil cytoplasmic antibody (ANCA) was positive. A diagnosis of granulomatosis with polyangiitis was made, and immunosuppression was initiated for treatment of this ANCA-associated vasculitis. At 6 months of follow-up, the patient’s symptoms had abated; repeat CT imaging showed resolution of lung nodules and stable facial findings.

