



Shoulder Examination Inspection & Palpation - Everything You Need To Know - Dr. Nabil Ebraheim
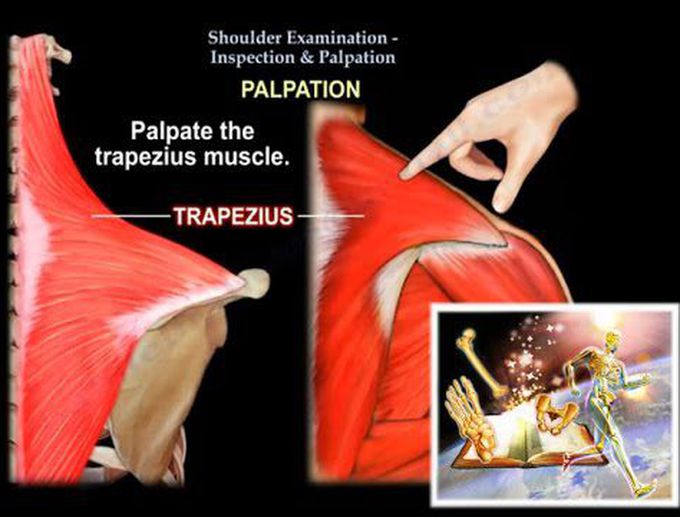
Dr. Ebraheim’s educational animated video describes shoulder impingement examination and palpation, explains its signs and symptoms, etiology, prognosis, and treatment options in a simple and easy way. When you examine the patient with a shoulder problem, you need to look at the shoulder. Inspection of the shoulder is not as easy as inspection of the lower extremity. Start looking at the muscles, if they are small, atrophied, wasted or big. So if you look at the back and you find that the suopraspinatus is wasted, then you should start thinking about the suprascapular nerve, if the patient is young, or maybe a couple of tears if the patient is old. Then you start inspecting the deltoid, check its size and compare it. Then the biceps, flex the elbow and test it, rule out the tear, biceps tear maybe associated with rotator cuff tear. Look at the pectoralis and the axillary fold, make sure that the folds are the same on both sides. Look for deformities: - Are the shoulders at the same level? - Does the patient have AC separation? - Are the clavicles sticking out? - Does the patients scapula winging? And what type of winging? Is it a medial or a lateral winging? Then we look at the scars: the scars of previous surgeries and where is it located, because we may incorporate these scars in our future surgery. Then we look at the swelling, it’s hard to see but sometimes you can see it. Also we look at the skin, do you have redness around the shoulder? Palpation: You are going to palpate all the bony prominences around the shoulder and also the important muscles. Start from the sternoclavicular joint, to the clavicle, to the AC joint, the AC joint can be a source of pain, the you go to the coracoid process, to the axillary crease, then try to role the finger to find the biceps, and find out if you have a biceps tenderness or not, then palpate the pectoralis tendon at the axillary fold, tenderness over the leading edge of the acromion can be an impingement syndrome or a rotator cuff problem, palpate the deltoid, the trapezius, then palpate for trigger points: which comes from the levator scapulae muscle and physiotherapy will make a big deal about it, then you make the decision: is it a neck problem or a shoulder problem. Don’t miss the cervical spine: palpate the posterior cervical spine and examine the movement of the spine, check the spurling maneuver. Palpate the spine of the scapula the medial border of the scapula, the lateral border of the scapula; in slap lesion we have pain in the posterior edge of the acromion in the soft spot. So as you can see It is a 360° palpation, and don’t miss the cervical spine. You may actually start the examination by examining the neck first, then the trapezius, then the clavicle, and start the 360° examination. Try to check for any crepitus or any swelling, go after the known area of anatomy that can elicit tenderness, that can lead you to the diagnosis.
