



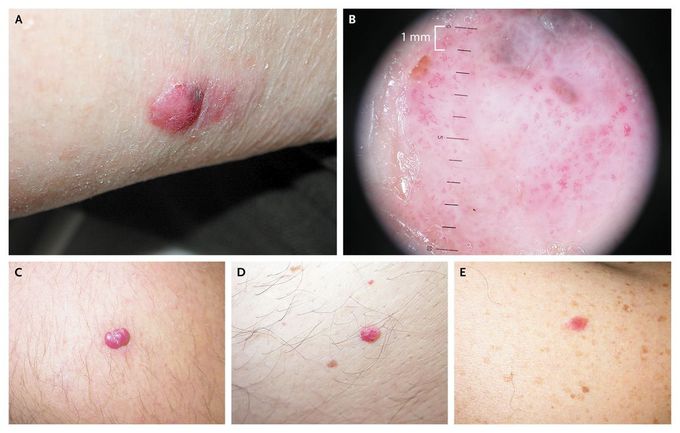
Red Melanoma
A 48-year-old woman presented with a 2-year-history of a red skin nodule with a blue-gray pigmented area at the 2 o'clock position on her left upper arm (Panel A). Dermoscopy showed an irregular, reddish, diffuse pigmentation, a focal regression with irregular brown-gray globules (corresponding to the blue-gray pigmented area), and a diffuse polymorphous vascular pattern (Panel B). Once the melanocytic nature of the lesion was clarified with dermoscopy, it was excised. Histopathological examination confirmed the clinical and dermoscopic diagnosis of amelanotic melanoma, with a Breslow thickness of 3.9 mm. After excision of the nodule, a biopsy of the sentinel lymph node was performed, and metastatic melanoma was detected. Axillary lymphadenectomy was performed, and owing to the detection of cerebral and skeletal metastases the patient also received adjuvant chemotherapy. Amelanotic melanoma may appear to be similar to many common benign skin lesions (e.g., pyogenic granulomas [Panel C], angiomas [Panel D], and dermal nevi [Panel E]) and is therefore often erroneously treated with the use of diathermy or laser vaporization. This case highlights the need for careful consideration of the differential diagnosis of red nodules; further histopathological investigation should be conducted if cancer is suspected. Adone Baroni, M.D. Vincenzo Piccolo, M.D. Second University of Naples, Naples, Italy source: nejm.org
