



Superficial Abdominal Reflex
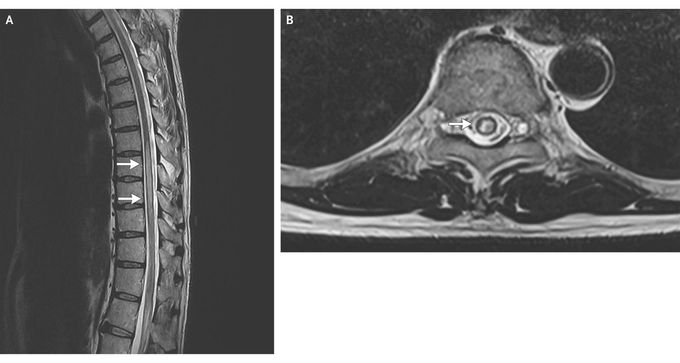
A 59-year-old man presented with a 5-day history of bilateral lower-limb numbness, unsteadiness of gait, and urinary incontinence. On examination, he had bilateral lower-limb weakness (strength, 4/5), with normal tone and deep-tendon reflexes. The plantar reflexes were normal bilaterally. There was a sensory level at T10. Visual evoked responses were delayed on both sides. Absence of the superficial abdominal reflex on the right side (see Video) correlated with the finding of a hyperintense lesion in the spinal cord on T2-weighted magnetic resonance imaging, spanning T7 to T10 (Panel A, arrows), predominantly on the right side (Panel B, arrow). The analysis of the cerebrospinal fluid was normal. A test for anti–aquaporin 4 (NMO-IgG) antibodies was positive. He was given a diagnosis of neuromyelitis optica and treated with intravenous methylprednisolone for 5 days. Azathioprine therapy was also initiated. At 1-month follow-up, his neurologic deficits had resolved completely except for some residual sensory symptoms. The superficial abdominal reflex can be used for localization of lesions in the thoracic spinal cord. It is elicited by gently stroking each of the four quadrants of the anterior abdominal wall. A normal response is a visible contraction of ipsilateral abdominal muscles. This reflex is now considered to be of minor clinical significance owing to the availability of neuroimaging studies and the difficulties in eliciting the reflex in multiparous women and patients who are anxious, elderly, or obese.
Tabarak Allah sir, you are so active you share best cases, may Allah give you good health and more knowledge
