



Microsurgical mgmt of a high-grade brain AVM in the central lobe after unsuccessful radiosurgery
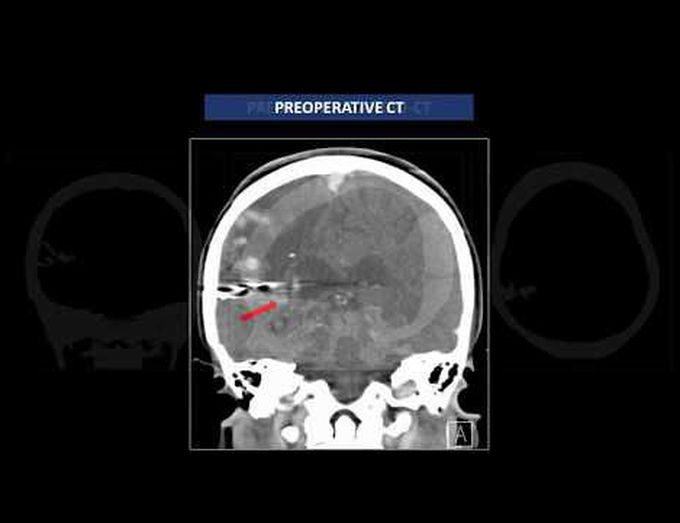
Division of Cerebrovascular and Skull Base Surgery, Center of Neurology and Neurosurgery Associates (CENNA), Hospital Beneficência Portuguesa de São Paulo, Brazil The recommendation for the great majority of high-grade brain arteriovenous malformations (bAVMs) is observation, except for those patients with recurrent hemorrhages, progressive neurological deficits, steal-related symptoms, or AVM-related aneurysms, for whom intervention should be considered. These are general recommendations, and the decision should be made on an individual basis. Surgical resection of an AVM in the central lobe may cause postoperative sensorimotor deficits since this anatomical region includes the pre- and postcentral gyri on the lateral surface and the paracentral lobule on the medial surface. The authors present a patient with a ruptured high-grade bAVM in the central lobe who underwent previous surgery for hematoma evacuation and previous radiosurgery, and whose indication for reoperation was proposed based on progressive hemiparesis. Microsurgical resection was possible after a wide frontoparietal craniotomy, which made all the nidus borders accessible. This case illustrates the anatomy and surgical technique for large nidus AVMs in eloquent areas, showing that complete microsurgical resection is possible with good clinical outcome.
